| 00:07 | This is lecture seven of Cellular And we're gonna briefly review information on |
|
| 00:17 | modulatory systems and a lot of it is the review for those that's taken |
|
| 00:23 | nurse on. I just want to sure everybody remembers this sometimes uh repeating |
|
| 00:28 | makes you really good at things and them and understanding them for the future |
|
| 00:33 | those that have not taken my course they have taken a different version of |
|
| 00:37 | course or some part of that is uh a quick review as well. |
|
| 00:43 | , from the very beginning, I that when we talk about the glutamic |
|
| 00:47 | g allergic systems and glutamate producing neurons gap producing neurons, we said that |
|
| 00:53 | dispersed throughout the brain. That means the somos of these neurons are gonna |
|
| 00:57 | found everywhere. Spinal cord and hippocampus frontal cortex and uh occipital cortex, |
|
| 01:07 | systems. However, that if use systems for acetylcholine, for uh so |
|
| 01:16 | dopamine, for serotonin and norepinephrine are in such a way that the nuclei |
|
| 01:24 | produce these neurotransmitters are located in very zones. So these are very small |
|
| 01:33 | and these nuclei will contain thousands tens thousands, sometimes hundreds of thousands of |
|
| 01:41 | is depending on which system producing acetylcholine supplying acetylcholine from these nuclei into the |
|
| 01:49 | cord into subcortical areas. And from medial cepal nuclei, this is the |
|
| 01:55 | follow the mental complex. This is sepal nuclei will send these acetylcholine signals |
|
| 02:04 | release these neurotransmitters diffusely throughout the And you can see that there is |
|
| 02:09 | significant uh difference in where these uh are located in the sense that they're |
|
| 02:19 | located in the brain. So the parts of the brain. So if |
|
| 02:22 | look at serotonin, we have rapid that is going to be producing all |
|
| 02:27 | the serotonin available in the brain, . It's locus cus and for dopamine |
|
| 02:34 | , it's vent to glutol area as as substantial nigra. Now, when |
|
| 02:42 | looking at the cholinergic system, let see if I can get rid of |
|
| 02:46 | style bar. When we're looking at cholinergic system, this is acetylcholine as |
|
| 02:52 | were talking about and it has a supply in this uh basal forebrain |
|
| 03:00 | which is co of telencephalon or the , medial and ventral to basal ganglia |
|
| 03:08 | basal ganglia is an important structure and movement. Uh paradigms. The |
|
| 03:15 | of these are mostly unknown, but do know. So what does that |
|
| 03:21 | ? It's mostly unknown? We they're really diffused projections and it almost |
|
| 03:26 | resemblance uh of a para crime like of the release, but in the |
|
| 03:33 | and within the synapses, but very dispersed, it definitely participates in learning |
|
| 03:41 | memory. And that is important because is the system that gets compromised in |
|
| 03:47 | disease. And we know that once have Alzheimer's disease, there's a possibility |
|
| 03:52 | one of the first symptoms is going be loss of memory, short |
|
| 03:56 | followed by a long term memory. , on the other hand, uh |
|
| 04:01 | have this pontos phal tal complex which excitability of thalamic sensory relay nuclei. |
|
| 04:12 | if you can see that this complex really targeting subcortical areas and very heavily |
|
| 04:19 | the thalamus. Thalamus contain sensory nuclei uh vision for hearing some amount of |
|
| 04:27 | information processing. So that has a effect on this thalamic sensory relay |
|
| 04:35 | And this has a much stronger penetration the cortex, acetylcholine. Once it |
|
| 04:45 | released in the synaptic left, it broken down into the cline and acetic |
|
| 04:53 | , it gets transported back to I remember we talked about the transporters |
|
| 04:58 | glutamate transporters for Gaba. Well, are transporters for each one of the |
|
| 05:03 | that we're discussing here uh today at . And then that gets re synthesized |
|
| 05:09 | acetyl coa with the help of cline transferase produce acetylcholine. Then you have |
|
| 05:15 | transporter on the vesicle. So there a pre synaptic sodium cline cot transporter |
|
| 05:23 | it into the uh synaptic terminal and it gets transported and uploaded into the |
|
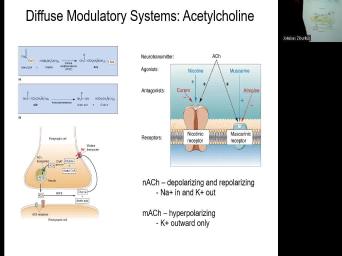
| 05:30 | for subsequent release. And the cns targets ionotropic. When we refer nicotinic |
|
| 05:40 | and metabotropic muscarinic receptors, we already what are agonists antagonists. If you |
|
| 05:47 | at the paper that talks about tagging means for pet imaging, pet scan |
|
| 05:54 | , it will tell you in uh like negative allosteric modulator things that we |
|
| 06:00 | discussed and you should have and sort your uh toolbox of understanding these are |
|
| 06:06 | , nicotine for nicotinic muscarine for muscarinic is a receptor channel. Muscarinic is |
|
| 06:14 | G protein coupled receptor. They will have their distinct antagonists. So, |
|
| 06:20 | Curari muscular muscarinic atropine, uh obviously, the agonist is nicotine and |
|
| 06:30 | comes uh as an active ingredient from . And so you will say, |
|
| 06:36 | , wait a second, then how you know, it's so harmful uh |
|
| 06:43 | tobacco and it's really the consumption of tobacco that's really harmful, especially the |
|
| 06:49 | or, or the vaping the nicotine on its own. If it's |
|
| 06:55 | it actually has shown some very interesting results in um Alzheimer's disease. And |
|
| 07:03 | some other experimental paradigms, it is is an addictive molecule. It is |
|
| 07:10 | uh probably one of the hardest sort available uh as a as as difficult |
|
| 07:18 | an addiction, but easier than I would say because it's still more |
|
| 07:23 | than available. So, but that's agonist. OK. Now, if |
|
| 07:28 | talking about activation of nicotinic acetylcholine it's permeable to sodium and potassium sodium |
|
| 07:35 | going to go and potassium is going go out. But the net effect |
|
| 07:38 | activating nicotinic acetylcholine receptor is depolarization. you activate muscular Nick receptor, which |
|
| 07:45 | G protein coupled, you're gonna have polarization because it's going to interact with |
|
| 07:51 | potassium channel. It's actually going to the nearby potassium channel through the G |
|
| 07:56 | cascade and it's going to cause hyper . So it has two opposing effects |
|
| 08:02 | at the level of the membrane. uh these effects are not as strong |
|
| 08:08 | some of the glutamate and Gabor signaling EP SPS and IP SPS that we've |
|
| 08:14 | discussing in the last couple of So, muscarinic receptor activation can lead |
|
| 08:21 | through this what we call shortly to nearby potassium channel and open a nearby |
|
| 08:27 | channel nearby causing hyper polarization because potassium going to be e flex and it's |
|
| 08:34 | to be leaving the cell making the of the cell more negative catecholamines. |
|
| 08:42 | , catecholamines and all of these neurotransmitters we're discussing, especially the, I |
|
| 08:48 | , neurotransmitters, they have color and color is what they're responsible for, |
|
| 08:54 | function they're responsible for, what behavior for and also injury or impairment in |
|
| 09:01 | of these systems is typically associated with neurological disorders. So, impairment and |
|
| 09:08 | system is associated with Alzheimer's disease. . We're going to be talking about |
|
| 09:15 | impairments or uh dopamine dopaminergic system and uh we will notice that impairments and |
|
| 09:23 | are associated with motor neurodegenerative disorders such Parkinson's disease, but also potentially in |
|
| 09:34 | disorders such as schizophrenia. So you to think about these systems as these |
|
| 09:42 | have a limited number of neurons that that molecule, that molecule gets |
|
| 09:50 | In this case, you can see nigra again, is going to target |
|
| 09:56 | striatum right here and the subcortical areas the ventral tegmental area projections from here |
|
| 10:04 | dopamine, they're going to target the lobe in frontal cortex. It doesn't |
|
| 10:10 | as much penetration into the parietal occipital . So there is some specificity, |
|
| 10:15 | are differences between these an anatomy and diffused projections. So, dopamine |
|
| 10:22 | mood attention and visceral function impairments and impairment and movement, potentially mood or |
|
| 10:33 | health diseases like schizophrenia, attention and . They are all coming from the |
|
| 10:39 | precursor tyra. And by all, mean dopamine or epinephrine and epinephrine thyra |
|
| 10:45 | a precursor that becomes dopa. Although becomes dopamine dopamine when it gets deco |
|
| 10:53 | , uh uh uh hy hydroxylase with beta hydroxylase gets removed, it becomes |
|
| 11:02 | epinephrine and then it becomes epinephrine through lot of uh enzyme. So this |
|
| 11:09 | the dopamine system. Now, this norepinephrine. So where's norepinephrine? We're |
|
| 11:19 | about norepinephrine and epinephrine. Ok. we somehow uh skip this slide. |
|
| 11:31 | again, if you look at the segmental area, it's obvious that it |
|
| 11:35 | targeting this area of telencephalon. Uh uh it's referred to as meso cortical |
|
| 11:45 | dopamine system, dopamine ergic projections from and substantia nigra axons project into the |
|
| 11:54 | right here. And it facilitates ini of the voluntary movements and degeneration of |
|
| 12:03 | substantial Migra and this stimulation causes Parkinson's . So I already mentioned that but |
|
| 12:11 | was a separate slide, actually, . Uh you have function that's regulation |
|
| 12:17 | attention, arousal, sleep, wake , learning and memory, anxiety and |
|
| 12:22 | , mood, and brain metabolism. lot of different functions are also overlapping |
|
| 12:27 | . And that's good because if you one of these neurotransmitters, so you |
|
| 12:31 | a reduction, there's a redundancy in some of these functions. So you |
|
| 12:38 | pathways that innervate very broadly. thalamus cortex, olfactory bulb, cerebellum |
|
| 12:47 | and all the way into the spinal here. Yeah, activation of norepinephrine |
|
| 12:57 | , typically the release of norepinephrine is , unexpected nonpainful sensory stimuli. So |
|
| 13:06 | really engages the brain. It's a of a no adrenaline, norepinephrine of |
|
| 13:12 | brain and to engage it, it's that is unexpected. Something that is |
|
| 13:18 | of ordinary, potentially a stressful it's not necessarily uh uh painful. |
|
| 13:29 | let's talk about norepinephrine, norepinephrine just like we saw with the acetylcholine |
|
| 13:36 | again, released. And what's different these systems of do dopamine, norepinephrine |
|
| 13:42 | they function through g protein coupled So, acetylcholine is unique in the |
|
| 13:48 | that it's the only one that has ionotropic and metabotropic signaling. All of |
|
| 13:54 | other means, dopamine norepinephrine serotonin, act through G protein coupled receptors. |
|
| 14:02 | the whole uh kind of a scheme release of norepinephrine, the synapse and |
|
| 14:09 | re uptake of the norepinephrine and reloading the neuropen release of dopamine, reloading |
|
| 14:18 | reuptake of dopamine and reloading of dopamine the vesicles to be released again. |
|
| 14:24 | what is shown here is uh illicit , cocaine will block the reuptake of |
|
| 14:33 | or norepinephrine. So that's why a of times you will hear in slang |
|
| 14:38 | it's an upper and that's because it stimulating or prolonging essentially the availability of |
|
| 14:46 | and upper and dopamine. Sort of no adrenaline all on uh uh off |
|
| 14:50 | brain and all of the functions uh them that we're talking about such as |
|
| 14:57 | , arousal, enhanced arousal, uh way a person communicates with you, |
|
| 15:03 | hopefully, no anxiety and pain because it wouldn't be very popular typically that |
|
| 15:10 | after a long weekend of consuming something this. Now, amphetamine also blocks |
|
| 15:16 | and dopamine reuptake and stimulates dopamine, cocaine. It's a little bit more |
|
| 15:23 | toward, toward dopamine, right. both of them will interact with |
|
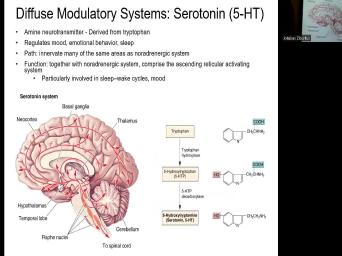
| 15:28 | but it will have a stronger effect dopamine serotonin system. It's derived from |
|
| 15:36 | , it's mood, emotions and So this is where we have the |
|
| 15:43 | that are coming from rapha nuclei. I always thought there were five, |
|
| 15:51 | it's four rapha nuclei that innovate many the same areas as neurogenic. So |
|
| 15:59 | don't know if I have subsequently a , but this is nor epinephrine neurogenic |
|
| 16:06 | . You can see it going like . And similarly, with serotonergic, |
|
| 16:13 | like this also going into cerebellum and into the spinal cord. So there's |
|
| 16:17 | significant anatomical projection overlap between these two . And therefore, it's likely that |
|
| 16:24 | going to be a functional, not anatomical but functional overlap. At least |
|
| 16:30 | overlap in certain behaviors of functions that regulate together with northern ergic system that |
|
| 16:37 | the ascending reticular activating system. It's an important system. This ascending reticular |
|
| 16:44 | system starts sending these slow weights and the brain, essentially preparing it to |
|
| 16:50 | asleep and enter into a different, uh different cycle as well as regulation |
|
| 16:56 | mood. All right. So you the tryptophan, it becomes five HCP |
|
| 17:03 | aroy tryptophan and then it becomes five or serotonin, which is abbreviated as |
|
| 17:10 | HT. And when we're talking about serotonin ssris or serotonin selective reuptake |
|
| 17:24 | Uh Here, actually, antidepressants are , for example, as tricyclics that |
|
| 17:31 | be affecting the transport reuptake of both and serotonin. And whenever you uh |
|
| 17:40 | the reuptake, what you're doing is making more of this norepinephrine and more |
|
| 17:45 | the serotonin available of the synapsis. we're available for, you're not making |
|
| 17:49 | of the molecule, you're just allowing to stay longer within the synapse, |
|
| 17:56 | spread spatially as well. FLUoxetine is antidepressant that will target serotonergic reuptake as |
|
| 18:06 | . And then we have ma O which are illustrated better in the subsequent |
|
| 18:12 | , which will actually target the breakdown . So now we're going to be |
|
| 18:17 | on the metabolism, it can actually the metabolism or the breakdown of these |
|
| 18:22 | . So if you block the this is happening inside the South. |
|
| 18:27 | you block the breakdown of serotonin or norepinephrine and serotonin, you have more |
|
| 18:34 | that molecule available. Now, most the antidepressant medications have uh have to |
|
| 18:44 | taken for a number of days, weeks, two or three weeks in |
|
| 18:49 | to exert a significant effect. And because if you think about it, |
|
| 18:55 | really kind of altering the homeostasis and metabolism of these very important molecules inside |
|
| 19:03 | brain. And if you especially talking ma O let me go to the |
|
| 19:09 | slide. If you were talking about ma O which breaks down serotonin, |
|
| 19:17 | you block the, if you block Ma Os, again, this adjustment |
|
| 19:24 | , blocking MA S and shifting the of that molecule even more of it |
|
| 19:29 | the synaptic cleft or more of it . Now, for synaptic terminal, |
|
| 19:34 | takes time uh equally. So to people when they take antidepressants and they're |
|
| 19:44 | antidepressants. And if they have side drowsiness or something else that they cannot |
|
| 19:50 | or they're getting way too sleepy then some other things that are not agreeing |
|
| 19:57 | them in the body, not necessarily in the brain, it could be |
|
| 20:01 | system. That's just, it's not to get off of it. |
|
| 20:07 | if you were having a pleasant again, it will take like two |
|
| 20:13 | to two weeks to three weeks to, to, to restore that |
|
| 20:19 | , to restore that what we call normal dynamic range or the one that |
|
| 20:24 | the best with you. So this the pathway, the synthesis for |
|
| 20:31 | It has storage, you have a up into the vesicles released, you |
|
| 20:37 | activation of serotonin receptors. So there be norepinephrine receptor, serotonin receptors, |
|
| 20:44 | dopamine receptors, it's going to be and the receptor clear. So it |
|
| 20:50 | to the receptor by that, but doesn't stay bound forever. It actually |
|
| 20:55 | this receptor and then it gets So it can get reuptake by the |
|
| 21:02 | and get re uploaded. Also get and part of it instead of being |
|
| 21:07 | uploaded, gets hammered here, broken , metabolized by MA S. And |
|
| 21:14 | this is where when you're talking about uh pharmaceutical drugs or illicit drugs of |
|
| 21:20 | , that, that what you're understanding is that there's a whole system reap |
|
| 21:25 | poop cycling of these molecules and you interact with this system in different |
|
| 21:32 | Very interesting uh treatment that's emerging in society lately and has been accepted actually |
|
| 21:42 | FDA. Uh FDA has these caretaker protocols that allow people if the states |
|
| 21:51 | or uh clinical institutions, if they for people to use psilocybin mushrooms. |
|
| 21:59 | The fact of the matter is that , which is lysergic acid, which |
|
| 22:04 | synthetic acid, uh psilocybin mushrooms, comes from magic mushrooms or uh psilocybin |
|
| 22:14 | or whatever you wanna call it which is prevalent in Mexico and is |
|
| 22:20 | for the rites of passage traditionally and for ritual and recreational purposes. It |
|
| 22:30 | of these substances are interacting with the system. And what's really interesting from |
|
| 22:39 | latest treatments with psilocybin. So what you use psilocybin for, for the |
|
| 22:45 | things that you use serotonin medications? , depression, anxiety. The other |
|
| 22:52 | that psilocybin is being used for cited Linville trials in Harvard and some other |
|
| 22:58 | is for addiction. And what's interesting these clinical studies that are coming out |
|
| 23:07 | that it's one time use, one session. They require an individual for |
|
| 23:12 | , I think 6 to 10 hour with a guide and it's one session |
|
| 23:18 | seems to reorganize these systems. And there is emerging evidence that suggests a |
|
| 23:25 | synopsis of being formed following just one and exposure to drugs like psilocybin |
|
| 23:31 | or, or magic mushrooms. So not to say that uh LSD and |
|
| 23:36 | and all the other things do the thing. But that is really emergent |
|
| 23:40 | a, as an alternative. And an alternative because the person may have |
|
| 23:44 | treatment and they don't have to take pill two or three times a |
|
| 23:48 | They also take, have one treatment they report a change within days, |
|
| 23:54 | within hours. So they don't have wait for weeks and uh, we'll |
|
| 23:59 | where this goes, but this is emergent as a very interesting um alternative |
|
| 24:05 | treatment to all of these other drugs we discussed like tricyclics and such. |
|
| 24:11 | right, now let's move on into next lecture which is imaging of the |
|
| 24:21 | . And I believe that maybe one these, yeah, one of these |
|
| 24:25 | are a little bit out of got kicked in the front for some |
|
| 24:41 | and manipulate them. Um OK, we're gonna talk about imaging the brain |
|
| 25:16 | neuronal activity again to place ourselves reminding ourselves and also placing ourselves within |
|
| 25:24 | certain same level of understanding. So 2nd and 3rd section of this course |
|
| 25:29 | gonna be very heavily based on outside , also completely new material and these |
|
| 25:36 | of things are gonna keep coming up um over and over again. |
|
| 25:43 | So imaging the brain and this is reminder that historically, we really, |
|
| 25:51 | of all couldn't see neurons. So were concerned about staining neurons and glia |
|
| 25:56 | then we were had another obstacle is you cannot see through the brain. |
|
| 26:02 | if you cannot see through the you cannot image deep structures. And |
|
| 26:08 | there was a technique, this new method that was created, it clarifies |
|
| 26:13 | brain makes it transparent. You have absorbing lipids that are replaced with water |
|
| 26:20 | gel. And you use this green protein molecules that now can reveal really |
|
| 26:27 | regions of the brain. So it really help you visualize the brain in |
|
| 26:33 | . So this is what we can experimentally. So experimentally, we have |
|
| 26:38 | imaging, we have molecular imaging, have whole brain activity imaging and we'll |
|
| 26:43 | discussing these techniques. However, this of a imaging when we talk about |
|
| 26:50 | have two major types of imaging in brain. First of all, this |
|
| 26:54 | of imaging that is shown here is and a lot of what we discussed |
|
| 27:00 | far, self specific markers immuno to , molecular profiling, you could argue |
|
| 27:09 | molecular profiling tells you something about the of a specific neuron because it might |
|
| 27:16 | expressing or translating more of a certain , right. But in reality, |
|
| 27:23 | lot of the imaging bulgy stain, stain is static and we are interested |
|
| 27:30 | the functional imaging. And when you about functional imaging and we can do |
|
| 27:35 | static imaging at very high resolutions, can image single synopsis, you can |
|
| 27:42 | look at the cellular level. And really important is that for a long |
|
| 27:47 | , we have been doing recordings in . So we've been recording electrical activity |
|
| 27:53 | neurons like the potential, look the potential minus 65 mill volts. For |
|
| 28:01 | , here it goes through fluctuations and produces an action potential, another action |
|
| 28:09 | and another, it's quiet hyperpolarize, another action function, two action |
|
| 28:16 | Mhm. So we could record this activity and then we had the ability |
|
| 28:21 | stain the cells for with calcium dyes ions specific dyes. And what we |
|
| 28:26 | really interested in is how do we this activity and how do we correlate |
|
| 28:33 | image to the actual electrical activity in ? Because ultimately, this is the |
|
| 28:40 | real high resolution functional output of neurons changes in electrical potentials. But it's |
|
| 28:46 | the only one because this changes of potential do not necessarily reflect changes in |
|
| 28:55 | concentrations. They're correlated highly correlated, it is not what you are. |
|
| 29:01 | what you are recording, you're recording potential. So that's electrophysiology and what |
|
| 29:07 | noticed and what we know is neurons they're actively use oxygen, they use |
|
| 29:13 | lot of blood flow increases to that , the metabolism increases. So how |
|
| 29:18 | glucose they consume increases? We have . Um we can do slow and |
|
| 29:25 | imaging, we can do calcium imaging fluxes of calcium and neurons and |
|
| 29:31 | We can also image voltage that we'll about voltage sensitive dye imaging. We |
|
| 29:37 | also tag receptors with fluorescent or light and see how these receptors move through |
|
| 29:46 | tissue. And so we've discovered, example that remember we talked about these |
|
| 29:52 | receptors. In this case, I'm use ample receptors. So we talked |
|
| 29:58 | these synaptic receptors and these are the for suckers right there at the very |
|
| 30:10 | . These are the synaptic receptor that in the synapse. Ok. And |
|
| 30:16 | the neurotransmitter gets released, they get . So let's say these are. |
|
| 30:22 | then we talked last lecture, we that there are gaba receptors that are |
|
| 30:28 | of the synapsis, extra synaptic. I said they're responsible for the |
|
| 30:33 | And so we talked about the basic versus the Toni. So there are |
|
| 30:39 | amber receptors and other receptors that are synaptic outside the plane outside the |
|
| 30:46 | Then we have the tools to tag receptors, amper receptors. So we |
|
| 30:53 | the tools to visualize the synapse and have the ability to track these receptors |
|
| 30:59 | actually move into the synaptic space in activity dependent manner. And that movement |
|
| 31:07 | actually micrometers over milliseconds. So it's move. And that's how we can |
|
| 31:18 | track the receptor movement through the plasma f synoptic from extra synopsis into the |
|
| 31:25 | as well. So when we're talking static imaging, we're talking about x |
|
| 31:31 | and commuter computer tomography which is It's radiopaque material x-rays are two |
|
| 31:39 | They're great for bone structure. So you have your X ray done uh |
|
| 31:45 | bones for breakage or trauma in the . Uh computer tomography, which won |
|
| 31:52 | Nobel Prize in 1979 hunts fields and for it, computer tomography or CT |
|
| 31:59 | , essentially takes the X rays and X ray source beam now rotates |
|
| 32:07 | So instead of when you go now when you go to a dentist |
|
| 32:10 | , they take the three dimensional CT or three dimensional X ray, sometimes |
|
| 32:16 | scan uh but depending on what they using, but it gives you a |
|
| 32:23 | degree imaging. Now, using X and you have a digital reconstruction of |
|
| 32:29 | image. So you have a very imaging of living brains in three |
|
| 32:35 | In other words, it's noninvasive, individual goes into this apparatus to get |
|
| 32:40 | procedure done. And uh sometimes you want to inject contrast material that's called |
|
| 32:48 | very typical. One is iodine, example, into the blood vessels because |
|
| 32:54 | you can image the blood vessels which appear in darker color versus the tissue |
|
| 33:01 | the bone. So it gives you really good understanding of the structure in |
|
| 33:06 | dimensions throughout deep tissues. Actually using CT uh or computer tomography. Magnetic |
|
| 33:16 | imaging is based on hydrogen atoms responding the brain to perturbations of a strong |
|
| 33:25 | field and actually atoms creating their own fields and they resonate between high their |
|
| 33:33 | resonate between high and low energy states of jumping. And that's the resonance |
|
| 33:38 | in magnetic, there's magnetic coils just you saw. For example, here |
|
| 33:44 | have detectors for x rays. So have magnetic coils for uh recording MRI |
|
| 33:51 | , then not by computer to create imagery. What are the advantages of |
|
| 33:57 | over CT you get more detail with does not require x-ray radiation. So |
|
| 34:03 | all know that you have a uh limited number of times that you can |
|
| 34:10 | X rays during the year. But , it's a limited number of times |
|
| 34:14 | you can have these other procedures, pet scans because you're radioactively labeled. |
|
| 34:20 | it's limited the number of times that can have it a year. It's |
|
| 34:24 | dependent on your condition. Your health does not require brain sli image in |
|
| 34:31 | angle. So really good three dimensional of the structures takes about 15 minutes |
|
| 34:37 | compute the imagery. And after it's through the whole procedure, for |
|
| 34:42 | to do ac T scan of the brain may take about 45 minutes analysis |
|
| 34:49 | 15 minutes. And then a radiologist the same day or the next day |
|
| 34:55 | then you get some message from your or something that says that your scan |
|
| 35:00 | been read. And uh the report gets interpreted by an individual diffusion sensor |
|
| 35:10 | which is on the cover of the . It's water diffuses faster along the |
|
| 35:16 | axons rather than the cross. So a diffusion tensor imaging that's what was |
|
| 35:23 | . And diffusion tensor imaging is used reveal the connectivity of the brain. |
|
| 35:28 | really tracking more of the uh water huh imaging of the brain activity. |
|
| 35:37 | , this is still even if you doing this diffusion tensor imaging, it's |
|
| 35:44 | , anatomy, anatomy, no We want to get to the function |
|
| 35:49 | to get to the function, we to go to pet scans. And |
|
| 35:54 | is an image of the pet scan basic principles of imaging brain activity that |
|
| 36:01 | are detecting changes in blood flow and within the brain. In a clinical |
|
| 36:07 | , we do not have a resolution a single cell. Therefore, we're |
|
| 36:10 | at networks of cells that are being , active neurons and active neuronal networks |
|
| 36:16 | demand more glucose and more oxygen. , they will also be drawing more |
|
| 36:23 | to those active regions. And essentially we talk about pet scan, which |
|
| 36:29 | functional imaging or F MRI. And some experimental techniques that we'll discuss |
|
| 36:36 | we are kind of detecting changes in blood flow of blood supply to that |
|
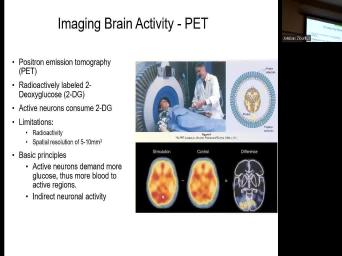
| 36:41 | or metabolism and supply to that So, positron emission tomography or pet |
|
| 36:48 | typically radioactively labeled two deoxy glucose. I do want you to open that |
|
| 36:56 | that I uploaded in the folders because will have a question for you about |
|
| 37:01 | article. A very general question And general question is such that right now |
|
| 37:07 | I'll tell you that it's radioactively labeled deoxy glucose and active neurons consume two |
|
| 37:15 | . We should start wondering which active all active nerves. So that is |
|
| 37:22 | . So it will show me all neurons in certain parts of the |
|
| 37:27 | But what if I'm interested in dopamine ? What if I'm interested in serotonergic |
|
| 37:37 | ? And the question that is a question for you guys is how can |
|
| 37:43 | image, how can you get to a single cell but to a cell |
|
| 37:53 | specificity in pet scans? So what , what are the, is |
|
| 37:59 | is it possible, is it possible image neurons with specific neurotransmitters that express |
|
| 38:10 | neurotransmitters? OK. So I'm gonna you ponder on this so we can |
|
| 38:15 | it uh next time we meet. but it's in the answer is in |
|
| 38:21 | paper that I've uploaded because again, all active neurons that are gonna light |
|
| 38:31 | and I'm interested in cholinergic neurons. , and is this like something that |
|
| 38:37 | an experimental setting and uh nonhuman for example of monkeys baboons or is |
|
| 38:46 | available in a clinical setting to And finally, you know, like |
|
| 38:52 | you think about it, we'll talk Alzheimer's disease, we'll talk about Alzheimer's |
|
| 38:58 | pathology. And one of the big of that we'll talk about in greater |
|
| 39:02 | is beta amyloid accumulation of beta amyloid the cells. Can, can we |
|
| 39:10 | these techniques to track been ambulance. we start picking up early before they |
|
| 39:19 | congregated into these deadly plaques that are essentially neurodegenerative. Can we start detecting |
|
| 39:29 | markers using these techniques? So it's necessarily the specificity of certain cells that |
|
| 39:35 | something but what about radioactively labeling certain ? How can we do that? |
|
| 39:42 | know how, how is this radioactive tag is gonna attach to a |
|
| 39:48 | of interest for us? That's, , that's food for thought limitations of |
|
| 39:56 | scanner be radioactive. You get injected radioactive solution and you're sitting around in |
|
| 40:05 | room for about 45 minutes when you the peak of your radioactivity and then |
|
| 40:11 | get summoned for imaging. So if it's a whole body scan, |
|
| 40:16 | will take over an hour. If a brain or a head scan, |
|
| 40:21 | may take 20 minutes, half an . It just depends basic principles are |
|
| 40:27 | that you have spatial resolution of 5 10 millimeters cubed. So 11 cell |
|
| 40:37 | 10 micrometers, the micro viewers. what you're imaging here is your |
|
| 40:52 | this kind of a cube, And this cube is let's say it's |
|
| 41:00 | by five by five millimeters. A mil millimeter is 1000 micrometers. So |
|
| 41:11 | 5000 micrometers. So you could technically 500 cells, 500 cells and 500 |
|
| 41:25 | . So maybe you can you can that math. What is 500 |
|
| 41:32 | It's a lot. I'm gonna do math. I'm curious if it makes |
|
| 41:40 | . No 125 million. So maybe that many cells in this cube, |
|
| 42:00 | maybe it's thousands of cells. Maybe did a, not a little bit |
|
| 42:09 | . Just so food for thought basic , active neurons will demand more glucose |
|
| 42:18 | that's more blood flow, active regions it's gonna get consumed there. |
|
| 42:23 | it's indirect neuronal activity. When we about direct neuronal activity, it's direct |
|
| 42:30 | in neuronal membrane potential. That is the gold standard and the comparison that |
|
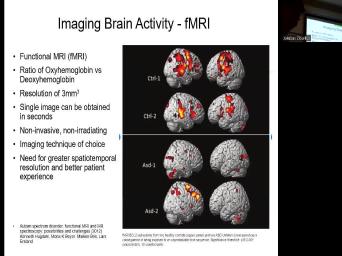
| 42:36 | making. OK. Now, functional resonance is ratio of oxyhemoglobin versus deoxy |
|
| 42:46 | . So neurons that uh are sucking a lot of oxygen, they will |
|
| 42:53 | the oxygenated hemoglobin and it will strip off the oxygen and will keep stripping |
|
| 42:59 | faster. So you can look at ratio of how much of it oxygenated |
|
| 43:05 | there's gonna be less of oxygenated hemoglobin the active areas. Changing that ratio |
|
| 43:12 | is now three millimeters cu single image be obtained in seconds or faster. |
|
| 43:20 | noninvasive, nonirradiated pet scan. You still say it's invasive, somebody is |
|
| 43:27 | something into you. It's imaging technique choice. Uh We do need greater |
|
| 43:34 | temple resolution, meaning we need still of these uh seconds. That means |
|
| 43:42 | activity is not real time. That that whatever your imaging happened a few |
|
| 43:48 | ago, maybe 15 seconds ago. that's not really ideal for neurons that |
|
| 43:55 | very fast and they communicate on the of milliseconds and hundreds of milliseconds for |
|
| 44:01 | most part. So better spatial spatial we can drive it down instead of |
|
| 44:10 | millimeters cube to 10 micrometers cube. would be amazing. And a better |
|
| 44:18 | experience because these procedures are difficult in , they have to go into the |
|
| 44:23 | , they have to get radioactive. have to sit in the coil for |
|
| 44:27 | minutes, maybe, uh cannot If you move, you have to |
|
| 44:32 | over the procedure. If you're it's difficult discomfort. If you're a |
|
| 44:38 | , you don't understand. In some , patients have to be anesthetized in |
|
| 44:43 | to go through that procedure. And just because they're so, so anxious |
|
| 44:47 | claustrophobic and going into these magnets and . Ok. So this is a |
|
| 44:55 | of resting state activity and this is discussion that you can read. If |
|
| 45:03 | go into a quiet room, lie and close your eyes, but stay |
|
| 45:06 | . What do you suppose your brain doing? And we've talked about it |
|
| 45:10 | my neuroscience course, because usually when show these brain maps, I get |
|
| 45:14 | question is, do we only use of our brain? Is that |
|
| 45:18 | And that is not true. You use different amounts of your brain depending |
|
| 45:22 | the tasks that your brain is But what happens when you're quiet. |
|
| 45:28 | your brain as busy? Are these maps that we're talking about neuronal network |
|
| 45:34 | ? Are they, are they still ? If your answer is not |
|
| 45:39 | you're probably in good company. So our discussions with various brain systems, |
|
| 45:45 | have described how neurons become active in to incoming sensor information or the generation |
|
| 45:49 | movement. And you can see this active cortical areas through the techniques that |
|
| 45:56 | just discussed, had an F MRI and now we can see resting state |
|
| 46:05 | . So we don't these techniques in clinical setting experimentally when we understood |
|
| 46:11 | oh my goodness, we can let person while they're in a pet |
|
| 46:15 | read something and their occipital lobe lights and we can have them listen to |
|
| 46:22 | and their temporal lobe lights out. this became really cool. How can |
|
| 46:27 | test like directly and more quicker pet is too slow? F MRI is |
|
| 46:33 | too slow but, but it's getting , it's getting there. And we |
|
| 46:39 | now understanding that there are certain regions are quiet and others that are actually |
|
| 46:44 | active. So an important question is if anything does the resting activity |
|
| 46:54 | And there is a obviously a difference the resting state of the brain and |
|
| 47:01 | state. There's also a difference in between different activities that we perform and |
|
| 47:07 | the brain is lighting up or showing these maps. So this activity what |
|
| 47:19 | shows basically is one possibility, both decreases and increases in activity are related |
|
| 47:25 | the task. For example, if person is required to perform a difficult |
|
| 47:28 | task and ignore irrelevant sounds, we accept the visual expect the visual cortex |
|
| 47:33 | become more active and the auditory cortex active, correct. You can block |
|
| 47:39 | out if you need to and you have to use a headphone sometimes. |
|
| 47:46 | we have the ability to shift this . And uh so what is, |
|
| 47:52 | , what is the default network? is the default state? So, |
|
| 47:59 | resting activity might vary randomly from moment moment and person to person and activation |
|
| 48:05 | with behavioral tasks would be so were on this random background. But it's |
|
| 48:15 | interesting discussion I'd like for you to . But two further observations suggest that |
|
| 48:21 | something fundamental and significant about the resting activity. First, the areas that |
|
| 48:27 | decreased activity compared to the resting state consistent when the nature of the task |
|
| 48:31 | changed. So it appears that the is showing decreased activity during behavioral tasks |
|
| 48:39 | always active address and become less active any task. So you have this |
|
| 48:45 | of a spatial interplay of up and activity and redistribution across different networks of |
|
| 48:53 | up and down activity. And sometimes , it's referred to as upstates of |
|
| 48:58 | versus downstate of activity, neuronal So the particular task does not seem |
|
| 49:06 | account for the activity changes. the pattern and the brain activity changes |
|
| 49:10 | consistent across human subjects. How consistent on this level. Meaning what? |
|
| 49:19 | five cubes millimeters, three cubed millimeters an approximate state. That activity is |
|
| 49:27 | you reading in front of pet scan me reading in front of pet scan |
|
| 49:32 | gonna light up the occipital lobe. , the the the devil is in |
|
| 49:38 | details, right. The devil is the connectivity. The devil is in |
|
| 49:42 | individuality of that connectivity that each one us has. And this type of |
|
| 49:48 | does not necessarily even reveal that. yeah, you can say it's |
|
| 49:52 | it's like all of the occipital lobes activated. But then if you get |
|
| 49:56 | more spatial resolution and if you get more temporal resolution will say, |
|
| 50:01 | that person's occipital lobe is dominated by Hertz frequency and the other one is |
|
| 50:06 | 37 and it's and it's constant, you can't have that speed of processing |
|
| 50:14 | using these imaging techniques. So another to imagine what a uh resting brain |
|
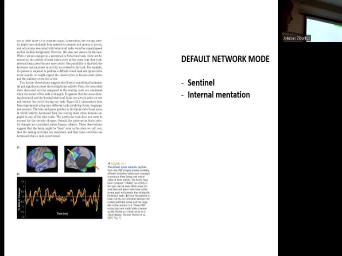
| 50:22 | does is this term that I really Sentinel State. So Sentinel state is |
|
| 50:30 | that the best analogy is uh a and duty is a soldier on |
|
| 50:38 | doing nothing on guard, really kind not doing anything right? Except that |
|
| 50:49 | are doing, they're waiting for something happen, they're waiting for somebody to |
|
| 50:54 | up at the gate and something like , right, if they're guarding |
|
| 50:58 | So this is kind of a similar you have this Sentinel state and you |
|
| 51:03 | compare the resting brain states to this of uh on guard but not necessarily |
|
| 51:10 | the tasks, not having as much the spatial specificity to what parts of |
|
| 51:16 | brains are activated, but definitely still activity and still performing with another school |
|
| 51:25 | is internal meditation. And that's I where if we could visualize each individual's |
|
| 51:32 | mentation, we would probably understand it's very different pathways and patterns of that |
|
| 51:38 | mentation of neuronal activity. That's what us individual and interpreting sensory stimuli and |
|
| 51:46 | our output out. You go to and you'll see a model and five |
|
| 51:52 | painting that model, they will all a different interpretation, which you'll |
|
| 51:57 | but their visual cortex is built the way and their motor cortex is built |
|
| 52:01 | same way. And you can even people that will be physically the same |
|
| 52:06 | and the same length of fingers. that, you know, you're not |
|
| 52:09 | biased towards the strokes of a pen something like that, you still have |
|
| 52:15 | interpretation and output individual output of, that picture of that activity that's happening |
|
| 52:25 | . OK. Now, how do put these images together? And actually |
|
| 52:29 | does that relate to the, the meng system in particular is that we |
|
| 52:37 | use, for example, multiple techniques order to understand which part of the |
|
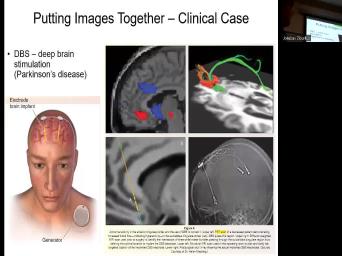
| 52:46 | is impaired. And you would do multiple techniques if you wanted to do |
|
| 52:50 | brain stimulation, that means you're implanting electrode inside the brain. That's why |
|
| 52:55 | is not the first one to do . It's been done for many, |
|
| 52:59 | years, but for different purposes. if this individual has Parkinson's disease, |
|
| 53:06 | disease, one of the symptoms of disease is tremors and abnormal movement of |
|
| 53:16 | in particular, but also limbs and becomes very difficult, it becomes very |
|
| 53:21 | to do almost anything to control your to pick up a cup of coffee |
|
| 53:27 | drink it. You cannot just basically if you have these continuous tremors. |
|
| 53:32 | for individual that have these tremors, doctor may suggest to have D BS |
|
| 53:38 | brain stimulation implants. And what they first do is they will take a |
|
| 53:44 | scan of the active areas of the that and in this right here and |
|
| 53:58 | the diffusion sensor imaging because you want determine what parts of the brain, |
|
| 54:03 | to connect it. So if you're to be implanting an electrode driving, |
|
| 54:07 | you want to avoid going through the , you may wanna go on a |
|
| 54:11 | or around the track. If you to get to this area of the |
|
| 54:17 | , finally you have here and uh and, and then you have a |
|
| 54:28 | . So you would do pet sensor , there's a structural MRI and you |
|
| 54:34 | the X ray because you kind of to see the location of everything with |
|
| 54:38 | to the to the bone of the . And all of these techniques are |
|
| 54:44 | be used in order to implant the for deep brain stimulation. Substantia Nigra |
|
| 54:51 | around substantia. Nigra is a target Debra simulation. Uh And what the |
|
| 54:59 | stimulation does is it has a control attached on the outside, it's a |
|
| 55:05 | . And when this controller picks up tremors, it activates the stimulating electrode |
|
| 55:11 | stimulating electrode produces a stimulus and it this abnormal shaking activity. So it |
|
| 55:18 | for individuals to get around much OK. And this generation the frequency |
|
| 55:25 | detection, it's all an iterative process a neurologist and clinician before you get |
|
| 55:31 | the mode that works best for you each individual may have a different stimulation |
|
| 55:36 | mode that they prefer. So these the more detailed descriptions of the imaging |
|
| 55:45 | that we've talked about. I just these for you. And um for |
|
| 55:53 | very last few minutes, we're gonna about experimental imaging and then I'm gonna |
|
| 55:59 | you a cool video and experimentally. in general, like I said, |
|
| 56:06 | interested in all of these scales, interested in the molecular of cellular, |
|
| 56:12 | scale circuit level scale mess copic which larger areas of the brain as is |
|
| 56:20 | here, for example, or Mac understanding how larger areas in the |
|
| 56:26 | it's not a sensory cortex and uh visual cortex may be interacting. And |
|
| 56:32 | , correlating this change in fluorescence because you are imaging activity, you're measuring |
|
| 56:40 | change in fluorescence typically. And that that change in fluorescence with electrical activity |
|
| 56:48 | become very important. And uh one the papers that I have uploaded for |
|
| 56:53 | talks about voltage indicators so that there dyes that are voltage indicators or what |
|
| 57:00 | call voltage sensitive dyes. Uh some them are for example, calcium |
|
| 57:07 | but they can be genetically expressed. so the paper discusses the advantages of |
|
| 57:14 | expressing these jetties versus the voltage sensitive that get applied onto the tissue that |
|
| 57:22 | gonna talk about here. So this a typical voltage sensitive dye. So |
|
| 57:28 | little squiggle, this is a molecule voltage sensitive dye. And if you |
|
| 57:34 | to record macroscopic activity of this area the brain, you'll actually apply the |
|
| 57:40 | onto this patch of the brain and dye is going to incorporate itself in |
|
| 57:45 | membrane of nerves full. But all it. I wanna know what happens |
|
| 57:52 | the allergic. So again, how we get to that specificity? But |
|
| 57:58 | interesting these little squiggles and once one these traces, I can't remember which |
|
| 58:03 | is green and red. Uh The the green one I believe is the |
|
| 58:08 | trace, the red one is the trace So here with these voltage |
|
| 58:15 | this is VM. And if you at delta F over F, you're |
|
| 58:23 | going to see a very similar pattern going to correspond 1 to 1 to |
|
| 58:34 | numbering potential changes. And these are advantages of voltage indicators. And in |
|
| 58:39 | voltage sensitive dyes, the disadvantage of sensitive dyes is that when you do |
|
| 58:46 | application, all of the neurons get with genetically express voltage indicators. There's |
|
| 58:55 | way to express those indicators in specific of cells. Again, we want |
|
| 59:01 | get the specific subtypes of subsets of in the clinical setting with pet |
|
| 59:07 | for example, tagging serotonin. And wanna get it in this experimental |
|
| 59:14 | But this experimental setting is something you do in humans cannot apply dye in |
|
| 59:19 | brain and image their brain. But is really cool. We used to |
|
| 59:23 | a lot of these studies with B set in dies. And the way |
|
| 59:26 | happens is that as I I always through the channel, these little squiggly |
|
| 59:35 | , the dyes change their confirmation as change their confirmation, they glow in |
|
| 59:40 | colors and give out a different delta over F. And just to demonstrate |
|
| 59:46 | the very end |
|