| 00:02 | There we go. I'm hoping that not bouncing around while I'm doing |
|
| 00:08 | So Okay, great. So here are, all 700 of us sitting |
|
| 00:18 | this classroom. It's just so Um, anyway, so what? |
|
| 00:23 | ? What? We're gonna continue on the cardiovascular system. Um, but |
|
| 00:28 | I do, just reminder we have do tomorrow. What's that? The |
|
| 00:33 | . Write your paper. Basically. make sure you get it in on |
|
| 00:36 | and then remember, next week you the peer reviews that you need to |
|
| 00:42 | . This will be, um you , you gotta make sure you do |
|
| 00:45 | five of them that you're assigned. you turn in your paper too |
|
| 00:49 | you're not able to participate. So becomes a zero. So you need |
|
| 00:53 | be able to that. Secondly, thing you guys did a calibration, |
|
| 00:58 | ? Was that the last one really ? Harder, wasn't it? |
|
| 01:03 | Now? Yes. No. You I wanna comment on that paper. |
|
| 01:09 | one wants to comment on the I just want somebody. Does I |
|
| 01:12 | him? You're there. It's a . Okay. Your mike is freaking |
|
| 01:25 | . Alright? I'll do this. we go. Thank you. |
|
| 01:29 | Basically, this paper was kind of middle of road paper. All |
|
| 01:31 | so it had some good points that bad points. You probably figured that |
|
| 01:35 | . Probably after the second attempt was , Okay, there's a little bit |
|
| 01:39 | nuance to it then this. This be a paper that would probably average |
|
| 01:43 | 78 or so. You know, think this is what I graded it |
|
| 01:47 | . So if you found yourself always off the first time, maybe you |
|
| 01:53 | to temper yourself. Kind of think terms of All right, I'm not |
|
| 01:57 | to be nice. I'm not trying be mean. I'm just trying to |
|
| 02:01 | a proper assessment here, which is a really instructive thing to say. |
|
| 02:06 | the idea is that extremes are hard come by and most of this |
|
| 02:10 | I mean, it's real. Tell us something is garbage. It's |
|
| 02:12 | obvious when something is is really It's a little bit more difficult to |
|
| 02:17 | that middle of the road stuff. right? And so that's what's gonna |
|
| 02:20 | coming up. Um, I did an email from a student asking |
|
| 02:24 | um, sources and says the question , Is it okay if I use |
|
| 02:29 | source older than 2010? The answer yes. You can use a couple |
|
| 02:32 | sources older than 2010. You're not to 2010 and newer. But you |
|
| 02:40 | the majority of your sources becoming from stuff as opposed, opposed to older |
|
| 02:44 | . So you're not limiting yourself. idea is, I'm trying to move |
|
| 02:49 | what's new. All right, put in perspective. You're not going to |
|
| 02:52 | through your mom's closed toe where something , Because her stuff is from 1990 |
|
| 02:58 | ? You're gonna pick out new stuff people are gonna laugh at you. |
|
| 03:00 | you were in your mom's clothes as dumb example, I don't know why |
|
| 03:03 | thought about that one. I was , maybe because listen to the spinners |
|
| 03:08 | , which really is from the And I'm just picturing my mom's |
|
| 03:12 | which is really old. All there's gonna be a lot harder |
|
| 03:17 | I can see you guys were not the mood to be here, are |
|
| 03:21 | ? You didn't want to come did you? And you online? |
|
| 03:23 | guys were all watching YouTube, aren't ? We're getting thumbs up now. |
|
| 03:29 | , they're not paying attention. All , so let's talk about the E |
|
| 03:33 | g. You know, TCG is seen it. You watch enough movies |
|
| 03:37 | TV shows about medicine. So you've what a BCG looks like, |
|
| 03:42 | It looks like this thing right This is a perfect BCG. By |
|
| 03:45 | way. Most CCGs are not this perfect when you're looking at, um |
|
| 03:49 | right. And so the example I to use about this is I want |
|
| 03:54 | to think about football. And given I'm looking here, I don't see |
|
| 03:59 | lot of football fans here. I'm you guys not big football fans. |
|
| 04:03 | . All right. You ever watch football game? You know, someone |
|
| 04:07 | you, made you sit down and it like maybe the Super Bowl. |
|
| 04:10 | . Have you ever noticed that the angles none. Okay. Everyone knows |
|
| 04:19 | angles. Not always the same. not always from the same side. |
|
| 04:21 | like they're sitting there looking at the and watching the game from one angle |
|
| 04:25 | the time, right? Why is ? Why can't you see different |
|
| 04:29 | What do they have at the stadium allows you to see different angles? |
|
| 04:37 | cameras is what I'm looking for We could do charades here. |
|
| 04:42 | That's an old camera. You just to crank it. Now you just |
|
| 04:45 | your phone up. Maybe I should that. All right. Camera. |
|
| 04:51 | . So how many cameras do they on a football field? Do you |
|
| 04:55 | ? Lots. That's a good That's what I'm looking for is lots |
|
| 04:58 | we don't know. But you notice they if there's, like, a |
|
| 05:01 | call, you know, they go the replay booth, right? And |
|
| 05:05 | you have the announcer sitting there you know? Oh, well, |
|
| 05:07 | can see from this angle and then this angle, but this angle is |
|
| 05:10 | , but this angle you can But this one you can't and they're |
|
| 05:13 | showing you like five or six different of the play, right? So |
|
| 05:17 | E C G is like the cameras a football game. That was a |
|
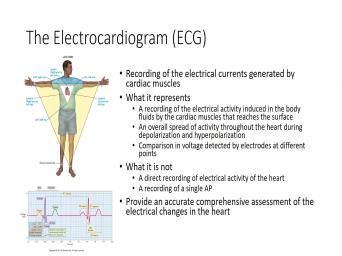
| 05:23 | way for me to get around to right. And really, what you're |
|
| 05:26 | is you're looking at the electrical activity the heart. So when you're talking |
|
| 05:30 | S E. G s, it's electrical activity of the heart. The |
|
| 05:32 | that those cardiac muscles are producing they have their own action potentials and |
|
| 05:37 | action potential spreading from cell to cell cell. And so you're looking at |
|
| 05:41 | of that activity at the same you're not just looking at a single |
|
| 05:45 | potential. Alright, so E G s do not record single action |
|
| 05:49 | . They record the refraction of the activity of the heart. As |
|
| 05:54 | you know, reflects throughout the I should say the reflection, not |
|
| 05:58 | refraction. All right, so when looking at this, we have to |
|
| 06:02 | that's what we're seeing. All Now the way that we're gonna we're |
|
| 06:06 | we're gonna see this in the next slides and you can kind of see |
|
| 06:09 | has this triangle looking thing in our cartoon. And what this represents is |
|
| 06:14 | the leads air actually located, all ? And so what you're not doing |
|
| 06:18 | you're not looking specifically at the hardened heart. What are you doing? |
|
| 06:22 | looking at the heart from different angles what you're doing is you're looking at |
|
| 06:28 | pulses from those angles, and then take a composite of all of these |
|
| 06:32 | angles, and it gives you this right here. All right. It |
|
| 06:37 | shows you what that comprehensive view of that electrical activity looks like from all |
|
| 06:43 | different angles. All right, so gives you a complete picture of what's |
|
| 06:47 | on. All right, so it's comparison, the vulture voltage detected by |
|
| 06:52 | of the different electrodes that air So what we call these electrodes refer |
|
| 06:57 | them as leads. And these leads connected in very specific locations. Good |
|
| 07:01 | . You don't need to know all locations, but this kind of shows |
|
| 07:04 | a picture of one where you can how it's like, Look up there |
|
| 07:08 | the top left corner. You can that I have a lead at each |
|
| 07:12 | . And so basically, I'm looking the heart between those two points and |
|
| 07:17 | electrical activity, and you could see each of these different leads give you |
|
| 07:22 | sorts of views in terms of what electrical activity looks like. All |
|
| 07:26 | so there's 12 leads and all. one of the wrist went the leg |
|
| 07:30 | then six across the chest. And can see this is the thing showing |
|
| 07:33 | with the chest how they're kind of up on there, right? So |
|
| 07:37 | , I'm not gonna ask you I'm gonna ask you what is V |
|
| 07:39 | ? Looks like what is V six like, you know, that's that's |
|
| 07:42 | important. For if you ever taken BCG class, then you'll have to |
|
| 07:46 | all that stuff. All right? not even gonna ask you what a |
|
| 07:50 | one looks like, What or what bad E. C G looks |
|
| 07:54 | All I want to understand right now that this represents the total electrical activity |
|
| 07:59 | the heart. And if you look this, each of these little parts |
|
| 08:03 | the E C G represents something as of the cardiovascular events that are |
|
| 08:09 | All right, so we're asking the we talked about yesterday or Tuesday. |
|
| 08:14 | said, Okay, the heart goes these periods of contraction and relaxation. |
|
| 08:18 | have two Atria. We have two . The eight year contract Together, |
|
| 08:21 | ventricles contract together. There's a pulse begins in the a V or |
|
| 08:25 | The essay No travels to the A , no doubt travels down the bundle |
|
| 08:28 | his up through the parking G fiber to all the contract ourselves to create |
|
| 08:33 | , this Siris of contractions, from atria to the ventricles to move blood |
|
| 08:37 | the body. So if that's all , how or what does this look |
|
| 08:43 | ? What does this is? How this represented electrically, All right. |
|
| 08:46 | that's what the BCG does. It says, Look, if I look |
|
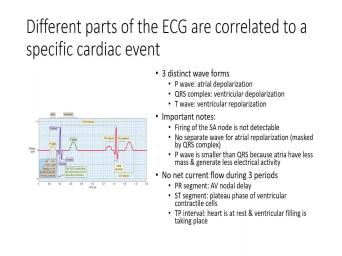
| 08:49 | this, I can see I have wave forms you can see there's the |
|
| 08:52 | wave, the QRS wave, the wave. Then there's this period of |
|
| 08:55 | in the P wave. The Q s t t and just repeats over |
|
| 08:59 | over and over again. And if watch enough, uh, hospital TV |
|
| 09:03 | or hospital movies, you've seen a where someone's lying on the bed. |
|
| 09:07 | doctor is looking very concerned, and machine in the bad going beep people |
|
| 09:12 | . And that's what you're looking at E. C G. All |
|
| 09:17 | so what do these way forms Well, the PIF wave represents the |
|
| 09:23 | polarization of the muscles of the So when they begin to be polarized |
|
| 09:28 | that they can create a contraction, what you're watching. Is that electrical |
|
| 09:31 | spread over all that muscle? All , The QRS represents ventricular deep |
|
| 09:38 | So that's the spread of the pulse the ventricular portion of the heart. |
|
| 09:44 | then the T wave represents that ventricle polarizing and returning back to rest. |
|
| 09:50 | are we missing? Re polarization? huh. Okay. Well, |
|
| 10:03 | Does the atrial re polarized? What you think? Should it re |
|
| 10:07 | Have a deep polarizes. Should have polarized. Yeah. Yeah. So |
|
| 10:11 | right. So that that should be Okay, Yeah, that kind of |
|
| 10:14 | sense. If it's contracting at some , it has to relax. So |
|
| 10:18 | is it? All right, I'll tell you where it is. |
|
| 10:21 | up there. You just can't see . I have three Children. I |
|
| 10:25 | four kids. I have three All three boys look exactly like |
|
| 10:29 | All right. They're just small versions Dr Wayne's. Put them in a |
|
| 10:32 | like this and jeans right here. think I shrunk down. I got |
|
| 10:35 | bunch of mini Mees. All Well, the 13 year old is |
|
| 10:39 | to look more my size. you know, you get the just |
|
| 10:44 | If I brought my youngest son in , he's a little bit shy and |
|
| 10:48 | put him in front of this There's only eight of you, but |
|
| 10:50 | still freak out there. There's six you, plus ta, right? |
|
| 10:55 | when you could imagine this whole room , he'd be like, you |
|
| 10:59 | and he would zip behind me and behind me, right? And then |
|
| 11:02 | try to move. And what would did Move with me. If I |
|
| 11:05 | to turn, he'd hide behind You'd never be able to see |
|
| 11:08 | You might see him peek out every and then. But if I really |
|
| 11:11 | of like, tried to go real , you just stay right over |
|
| 11:13 | Just wouldn't move. Well, guess ? That's where the the atrial re |
|
| 11:19 | is. It's hiding behind the R s. All right, It's |
|
| 11:24 | there because the atrial muscle is so relative to the ventricular muscle, you |
|
| 11:31 | get to see its activity. The atrial muscle. Remember what I |
|
| 11:36 | ? is not so much about propelling through the body, so there's muscle |
|
| 11:41 | . But it's not really strong All it has to do is squeeze |
|
| 11:44 | to get the blood from the atria the ventricle. It's not even all |
|
| 11:46 | blood that enters into the atria that that. We're going to see more |
|
| 11:49 | that today, right? Instead, we have is we have this really |
|
| 11:54 | muscle, the ventricle, which is for squeezing the blood out of the |
|
| 11:58 | and into either the systemic circulation or the pulmonary circulation. It's a |
|
| 12:03 | strong muscle, which is what gives this very big wave. And in |
|
| 12:07 | , if you think about it, what we said. We said the |
|
| 12:09 | of hiss went down the middle of septum and then spread upward and outward |
|
| 12:14 | the ventricular muscles and look at what wave does. It goes down then |
|
| 12:18 | , then down again. And what represents is that movement of that wave |
|
| 12:22 | electrical impulses traveling down and back and . And that's why you're seeing going |
|
| 12:27 | and down all right? It's a of actual direction. All right, |
|
| 12:35 | , you don't see the s a firing. You see a point where |
|
| 12:38 | firing up there? I mean, labeled it, but do you see |
|
| 12:41 | actual blip or anything on there? . So the s a node is |
|
| 12:45 | series of action potential. They're very small and undetectable relative toe all |
|
| 12:49 | muscle that's there. Now, you also see that there's these periods of |
|
| 12:54 | where there is no current taking All right, we have names when |
|
| 12:58 | call the PR segment. Right? have the S T segment, and |
|
| 13:02 | we have the teepee interval. Sounds something that you do in the |
|
| 13:09 | That was funny. You're supposed to my wife. I do jokes like |
|
| 13:13 | . That's so soft. Mark, like, yeah, you married |
|
| 13:16 | E was like that. Come 20 p interval. I mean, |
|
| 13:21 | funny, isn't it? Yes. getting to get. See? Now |
|
| 13:25 | starting to do it. Okay? can laugh at stuff like that when |
|
| 13:29 | have kids. Then you can put the stoic face and pretend like nothing's |
|
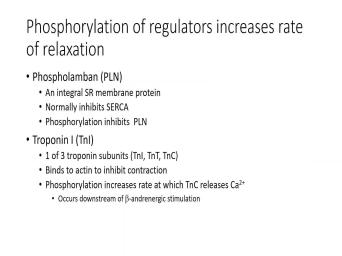
| 13:32 | . But now it's OK. What? Each of these represents is |
|
| 13:37 | period of time where that electrical activity happening, right? So if I |
|
| 13:42 | eight year old deep polarization, that's that wave of activity that's causing the |
|
| 13:47 | to contract. And then during that before you muscle relaxes, then you're |
|
| 13:54 | having electrical activity, right? So polarization represents the period of contraction. |
|
| 13:59 | polarization represents a period of relaxation. in between, what do you you're |
|
| 14:03 | a state of? You're in a of contraction. There is no |
|
| 14:07 | right? And then between the eight contracting in the ventricle contracting, you |
|
| 14:11 | this period of rest, and then you have in the ventricles. You |
|
| 14:16 | a period of contraction. The Q s. You have the teepee, |
|
| 14:19 | is a period of relaxation. But those two things, you're in a |
|
| 14:23 | of contraction, so there's no So it's a period of electrical |
|
| 14:28 | and that's what those represent. The represents the rest between the period of |
|
| 14:33 | , when the ventricles contract and then . There's TP is relax ation, |
|
| 14:40 | then the P wave, remember, the period of atrial contraction in the |
|
| 14:45 | step. So that's a long period diacetyl that's taking place, but in |
|
| 14:51 | teepee period. All right, I mentioned this on, um, |
|
| 15:02 | about the valves. Alright, I'm reiterating it. I guess I had |
|
| 15:06 | in the wrong order something, or is how I used to teach |
|
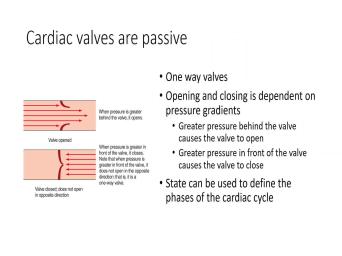
| 15:09 | I don't know, but this is I put here. Remember, those |
|
| 15:12 | in the heart are one way Alright. All their opening and closing |
|
| 15:17 | is they are not dependent upon electrical . They're dependent upon pressure. Grady |
|
| 15:23 | right. So when the valves it's because the pressure on the backside |
|
| 15:28 | the valve becomes greater than the pressure the front side of the valve. |
|
| 15:32 | right. And then when the valve , it's a function of the pressure |
|
| 15:36 | the front side of the valve being than the pressure on the back side |
|
| 15:39 | the graph valve. It's not because heart decided all of a sudden time |
|
| 15:43 | open the gate and let the blood its solely a function of pressure. |
|
| 15:48 | we need to be kind of aware those pressures. Alright. Thes states |
|
| 15:53 | the vows being an open and closed us to see the different phases of |
|
| 15:58 | it's called the cardiac cycle and with majority of today's lectures on is gonna |
|
| 16:03 | on this cardiac cycle. I'm gonna you a graph in a couple of |
|
| 16:10 | , and you're all going to freak because it's a graph. All |
|
| 16:13 | But if you understand this graph that going to show you, you're gonna |
|
| 16:20 | everything you need to know about the and the truth. ISS is the |
|
| 16:24 | isn't that hard. Don't tell All right, let the people freak |
|
| 16:31 | . Who don't like graphs. The of us could go. This is |
|
| 16:35 | . Oh, I'm freaking out, . Okay, that's cool. All |
|
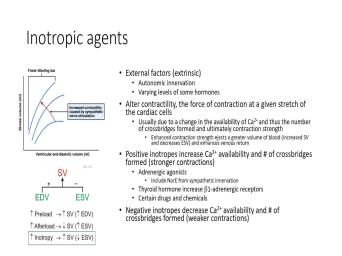
| 16:41 | , So what is the cardiac Simply put, the cardiac cycle is |
|
| 16:46 | period of sisterly versus diastolic. All , And so this is kind of |
|
| 16:50 | big picture right here. Forward sisterly Sicily means contraction and emptying. It's |
|
| 16:55 | period of time when that spread of is occurring and the muscle begins to |
|
| 16:59 | to propel the blood forward. What diastolic? Diastolic simply means relax |
|
| 17:04 | So at this point, this is muscle relaxing because the muscles relaxing that |
|
| 17:08 | for the flow of blood into that . And it's a period of re |
|
| 17:15 | . Alright? And so your heart gonna alternate between these two states and |
|
| 17:19 | already know this, right? You the thump? Thump, thump, |
|
| 17:21 | . What are you doing? You're and relaxing. Thump, thump, |
|
| 17:24 | , relax, Squeeze, relax, , Relax. That's what your heart |
|
| 17:27 | all day long from now until the you die. And that's a true |
|
| 17:32 | in it. When you die, heart's not gonna be doing that. |
|
| 17:39 | huh. All right, now, we think Assistant Lee in Diastolic, |
|
| 17:44 | typically think of the ventricles. because the ventricles are doing all the |
|
| 17:48 | of pumping the blood out into But the atria have the same cycles |
|
| 17:55 | sisterly and die asleep. But when talk about sisterly, that's if you |
|
| 17:59 | me say okay insistently, you should think ventricular sisterly. If you hear |
|
| 18:04 | say diocese, you immediately think ventricular . When I prefix it with |
|
| 18:09 | Then you know I'm specifically talking about , sisterly or atrial joyously. There's |
|
| 18:15 | that's just the way the nomenclature All right, But you can see |
|
| 18:19 | our little circle out here and the circle. We have ventricular system. |
|
| 18:23 | showing you a ventricular cycle and on inner circle, showing you the atrial |
|
| 18:28 | . All right. And you can do the two things line up with |
|
| 18:31 | other. Are sisterly atrial system in atrial or ventricular system where they align |
|
| 18:36 | or no, you can look at picture and tell me, Are they |
|
| 18:41 | up? No. You got atrial , occurring before ventricular Sicily. And |
|
| 18:47 | did I tell you yesterday, Or on Tuesday? What I say |
|
| 18:51 | atria have to contract. First, blood is pushed into the ventricles. |
|
| 18:55 | the ventricles push second. So there an order They're not lined up |
|
| 18:59 | Don't work together. The 28 year together, the tooth ventricles work |
|
| 19:04 | But the atria always precedes the ventricle terms of its contraction. All |
|
| 19:10 | now, depending on which textbook you to, they'll have a new inordinate |
|
| 19:17 | of phases for these this cycle. right. I think the freshman textbook |
|
| 19:23 | we used to use had, seven stages. I've seen books that |
|
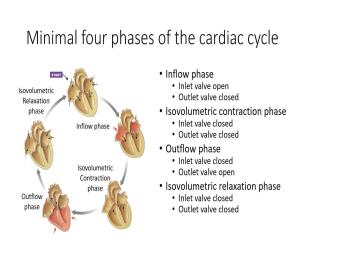
| 19:27 | nine stages. Some have five but ultimately it boils down to four |
|
| 19:33 | stages. And that's what this represents the four phases. Right? So |
|
| 19:38 | way you can think about is we an inflow phase and we have an |
|
| 19:41 | phase. That's really easy, Blood comes into the heart, blood |
|
| 19:44 | out of heart. That's pretty right? So real simple. In |
|
| 19:50 | inflow phase, that means you're inlet . The valve that is on the |
|
| 19:54 | on the front or on the back opens up and allows blood to flow |
|
| 19:58 | it into that chamber, the outflow into the venture. Cole has to |
|
| 20:03 | closed. Otherwise the blood would just going. But there's not enough force |
|
| 20:07 | be able to push it forward. that valve remains closed. We're going |
|
| 20:10 | see how this all works in just moment. Right? So in the |
|
| 20:13 | phase, we have the in valve the out valve closed. All |
|
| 20:18 | We're looking at the ventricle here. he ate your heaven in valve? |
|
| 20:23 | does not. Right. There is valve on the end. On the |
|
| 20:27 | side, it's just an out as far as it's concerned. All |
|
| 20:31 | , so in the outflow phase notice skipping here. I just want you |
|
| 20:34 | see this. So in the outflow , the inlet valve has to be |
|
| 20:38 | because there was not closed and blood flow backwards into the atria. |
|
| 20:43 | So the only value that's gonna be is the out valve. This allows |
|
| 20:46 | blood to go into circulation, So in flow allows blood to go |
|
| 20:51 | the ventricle. Outflow allows blood to the ventricle. Between these two |
|
| 20:57 | we have thes isil volumetric phases. is called a contraction. Phase one |
|
| 21:03 | called a relaxing phase. What do think is occurring during the contraction |
|
| 21:08 | What's happening to the muscles? The are contracting. And in the relaxation |
|
| 21:13 | , What's happening? See how this really, really complex and scary? |
|
| 21:18 | , it's relaxing, the muscles All right, but the key word |
|
| 21:22 | is isil. Volumetric. All which is why I pointed out first |
|
| 21:26 | a volumetric contraction phase is a volumetric ation phase. During the isil volumetric |
|
| 21:32 | phase, the muscles of the ventricles contracting, and there's fluid surrounding |
|
| 21:39 | All right, since I'm not allowed touch your stuff right now because |
|
| 21:43 | cove in and everyone's scared of I need you. Since I don't |
|
| 21:48 | anyone's name, I need you to your bottle, and I want you |
|
| 21:52 | squeeze it is hard you can to the fluid pop out. Go. |
|
| 21:57 | can't do it right now. The you can't do that is because you're |
|
| 22:01 | with the metal bottle. All I want you to do the |
|
| 22:03 | The same thing with yours. All ? Can you squeeze right? |
|
| 22:08 | the fluid wants to come out, it? Do you think you can |
|
| 22:10 | a force strong enough to make that come out? You could write. |
|
| 22:14 | the part that would give to allow fluid to escape the top? |
|
| 22:19 | so your top is acting as a in this case. And so what's |
|
| 22:23 | here is during the contraction phase, muscle is squeezing on that chamber just |
|
| 22:29 | you both squeeze on your bottles, ? The differences, her body a |
|
| 22:32 | bit weaker. It's basically being held the plastic years. Metal, |
|
| 22:36 | But you can imagine on this week bottle she can squeeze, and that's |
|
| 22:40 | push on. The fluid is creating inward pressure on the fluid is trying |
|
| 22:44 | drive. The pressure is trying to the fluid outward right, but it's |
|
| 22:49 | gonna leave until you create a strong pressure to overcome the pressure that's keeping |
|
| 22:55 | fluid in all right, and so this case, it happens to be |
|
| 22:59 | bottle cap. But on your the pressure that's keeping the fluid in |
|
| 23:04 | ventricle is the pressure, either in aorta that would be on the left |
|
| 23:09 | or the pressure in the pulmonary arteries would be on the right side. |
|
| 23:14 | if you can create strong enough pressure overcome that outward pressure that that back |
|
| 23:21 | , then that Zatz that period of where you're contracting. So in the |
|
| 23:26 | phase, blood flows into the ventricles the volumetric contraction phase of ventricle, |
|
| 23:33 | start contracting and creating greater and greater greater tension. In the outflow |
|
| 23:39 | the tension overcomes the back pressure so blood flows out. And then, |
|
| 23:45 | the muscles stopped contracting, they That valve slam shut, the change |
|
| 23:52 | volume or basically the muscle, There's no change in volume, so |
|
| 23:57 | what's occurring when you see is a . No change in volumes during that |
|
| 24:01 | . There's no change in the Just like when you squeezed on that |
|
| 24:04 | . There's no change in the volume the bottle was there. That makes |
|
| 24:10 | . Where have I lost you There is no change of when you |
|
| 24:19 | a change in volume. Look up . When do you think that volume |
|
| 24:22 | be changing? We'll squeeze it. . But just like what she |
|
| 24:27 | she squeezed on her bottle. Did change the volume inside the chamber? |
|
| 24:33 | . When she squeezed on her did she change the volume inside her |
|
| 24:38 | ? No, but it's trying to its attempting to, but there's not |
|
| 24:43 | strength being produced. Excuse me. enough attention being produced yet to allow |
|
| 24:49 | to happen. Once she produces either produced enough tension. Then what |
|
| 24:55 | Valve opens. Fluid flows out. changes. Yes. All right. |
|
| 25:03 | the question is, is there liquid not? Is there liquid there is |
|
| 25:07 | . Alright, so I'm gonna go the chart here and try to try |
|
| 25:11 | draw a little bit. We're gonna back to all this in greater detail |
|
| 25:14 | just smoke, but let me just of show you here. All |
|
| 25:17 | So we have our pan. Here's INC right there. That's your |
|
| 25:23 | Okay, so in your aorta, full of blood. Where does that |
|
| 25:28 | want to go? What? Where all liquid wanna go down? Where |
|
| 25:33 | the least amount of pressure. This is trying to flow back into your |
|
| 25:40 | ventricle. It's also trying to leave , And there's different ways that it |
|
| 25:44 | leave. There's different ways or different through which that blood could go. |
|
| 25:49 | just trying to find a way to out. All right, But that |
|
| 25:54 | resulting coincide that valve, which is there is closed. It won't let |
|
| 26:00 | out. But because you have pressure on that valve, you need to |
|
| 26:06 | enough pressure that causes that valve to in the direction you wanted to |
|
| 26:10 | Because remember what we said. Back slides. These valves are one way |
|
| 26:20 | . All right, so these are four phases. Now, if you |
|
| 26:30 | to, you can drop that same and you can put in there. |
|
| 26:35 | your cardiac cycle, right? And , we're just looking at the |
|
| 26:38 | We're ignoring the atria right now. ? So look what's happening in Diastolic |
|
| 26:45 | the ventricle is relaxed, What do have? All right, I'm gonna |
|
| 26:49 | up here at the start, in middle of die asleep. We have |
|
| 26:52 | flowing in and even further in to ventricle because the ventricles relaxed. We |
|
| 27:01 | this valve open. So blood flows the ventricle, all right, And |
|
| 27:09 | isil volumetric. And that's what it's . You see, it's like the |
|
| 27:11 | going in. No, look, keeps going in. That's what that |
|
| 27:14 | arrow is showing you. And then say, All right, now the |
|
| 27:17 | begins to contract. That's at What happens? That valve slam |
|
| 27:24 | Right valve, slam shut. Fluid leave backwards. It can't leave |
|
| 27:31 | so the volume stays the same. tension is building up. When the |
|
| 27:37 | becomes great enough, Then we become enter into the outflow phase. Those |
|
| 27:41 | still insistently right now, the blood depending on which side of the heart |
|
| 27:46 | looking out through the order through the arteries. And then volume is leaving |
|
| 27:52 | ventricles. Squeeze on that chamber. volume of the chamber gets smaller, |
|
| 27:56 | then the muscle relaxes, which causes valve to slam shut again. |
|
| 28:04 | So there's this period of time where volume inside their stays the same. |
|
| 28:10 | then the fluid builds up in the . And then when that pressure inside |
|
| 28:14 | atria becomes large enough, boom ! opens up that valve. And now |
|
| 28:18 | back to the inflow phase. That of makes sense. Are you |
|
| 28:27 | Be ready for the big the big big picture. Yes. Here we |
|
| 28:38 | . This bad boy right here, even blanking on the names right |
|
| 28:40 | It's like the Higgs I can't And you look at this thing and |
|
| 28:46 | gets a little scary, all And I want you to first, |
|
| 28:50 | know, just kind of take it for a second, and then |
|
| 28:51 | Okay? This really isn't as scary I think it is. And the |
|
| 28:55 | it's not so scary because you already this right there. That's your E |
|
| 28:59 | G. This right here is your cycle. We just saw that you |
|
| 29:03 | even see that we've labeled down there different stages of the cycle. All |
|
| 29:10 | . And then the rest of it's of simple. It's like, All |
|
| 29:12 | , well, we're gonna look at pressures inside the different chambers. All |
|
| 29:18 | ? We're gonna look at volume inside ventricle, and then this little part |
|
| 29:22 | here in the middle is the heart all right. So that's what that |
|
| 29:28 | chart is. And it's basically over . So this is time in that |
|
| 29:34 | . All right? Now, the step that we're looking at when we |
|
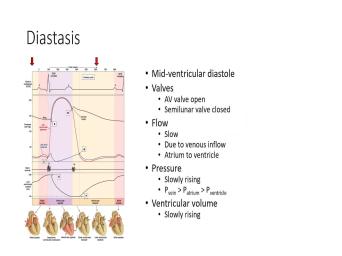
| 29:37 | at this cardiac cycle through this graph called DIA Stasis. Now, in |
|
| 29:42 | of these pictures, I'm gonna show . I'm gonna ask you to look |
|
| 29:45 | the valves, look at the flow the fluid look at the pressure and |
|
| 29:50 | the pressure is, and I'm gonna atyou in terms of the ventricular |
|
| 29:55 | All right, So here's our Where are we when we're talking about |
|
| 30:02 | Stasis? We're right here at the of the chart. But remember, |
|
| 30:05 | chart repeats itself, so it's also . Okay, so we're basically kind |
|
| 30:10 | in the there were looking at it this point, but this would be |
|
| 30:14 | next cycle. So dia Stasis is first stage. So if we look |
|
| 30:19 | the valves where in mid ventricular so mid ventricular diastolic, it means |
|
| 30:24 | ventricles are in their relaxed state, ? And so blood is flowing into |
|
| 30:30 | ventricles, and that's what's showing you here. The reason blood can flow |
|
| 30:35 | the intervals because the A V valve to be open, right? This |
|
| 30:39 | that inflow state. The semi lunar has to be closed. The reason |
|
| 30:44 | closed is because the pressure in the is greater than the pressure inside the |
|
| 30:50 | . All right, now we can that if we look over here, |
|
| 30:53 | aortic pressure. The red line down represents the ventricular pressure. The blue |
|
| 30:59 | right there represents the atrial pressure. notice the eight year pressure is higher |
|
| 31:06 | the ventricular pressure. So the reason flows from the atria to the ventricles |
|
| 31:11 | because fluid flows down at pressure grading high pressure. The low pressure, |
|
| 31:17 | the pressure and the atria was less the ventricle than blood, would want |
|
| 31:21 | flow the opposite direction. So the that you have greater pressure in the |
|
| 31:26 | is allowing the fluid to flow in direction. Now, why is there |
|
| 31:31 | pressure in the atria? No one to ask me that question. You're |
|
| 31:35 | fading on me. I can see in your eyes. Like pressure, |
|
| 31:39 | pressure sleep. Oh, yeah. reason is because remember, you just |
|
| 31:46 | blood out of the heart, pushed the blood. Remember you all |
|
| 31:48 | You don't know this shit. You about five liters of blood in your |
|
| 31:51 | , guys. About about 5.5 Females, You're about 4.5 liters |
|
| 31:55 | That's basically based on an average average average Every blah, blah, |
|
| 31:59 | blah. All right, But if push blood from my heart, I'm |
|
| 32:02 | a volume of blood out of my which pushes the volume in front of |
|
| 32:05 | forward which pushes the volume in front it. It forward? Yeah, |
|
| 32:08 | , all the way back around to heart. So what you've done |
|
| 32:10 | you basically pushed the bullets of blood to the lowest point, which happens |
|
| 32:15 | be your atria. So the pressure your atria went up the moment your |
|
| 32:19 | pumped, okay? And so that's you're seeing this flow into the |
|
| 32:25 | All right. Atria has higher pressure into the ventricles. It's a very |
|
| 32:30 | flow. You can see here. at the look at the slope. |
|
| 32:34 | not very steep, is it? . All right. Now the pressure |
|
| 32:42 | the ventricles is going up. if I put stuff into the |
|
| 32:48 | Increasing volume right? Not the space , but the amount of stuff |
|
| 32:53 | If I increase the amount of stuff , what happens to the pressure? |
|
| 32:57 | goes up. You want to visualize ? Go back to the example I |
|
| 33:00 | at the beginning of semester of a , right? I said, Here's |
|
| 33:03 | smart car. Put two people in car. There's not a lot of |
|
| 33:07 | in there, right, But there's pressure than there was when there was |
|
| 33:10 | . Put a third person in their . That space is still limited. |
|
| 33:15 | more pressure trying to get out, mawr even more. As you added |
|
| 33:19 | and more people, that's the same of things going on here. More |
|
| 33:22 | , I add in, the greater pressure inside the chamber. So you |
|
| 33:26 | the slow rise in terms of the . But the pressure inside the vein |
|
| 33:32 | driving the fluid into the atrium is than that in the a tramp. |
|
| 33:36 | pressure inside the atrium is greater than of the ventricle. And so what's |
|
| 33:40 | to the volume while it slowly rising the fluid moves from the atria to |
|
| 33:44 | ventricle? This is our first All right. Now I know this |
|
| 33:49 | very kindergarten is when I'm walking step step. But when we start putting |
|
| 33:52 | of the stages together, you can what's going on. Because what's gonna |
|
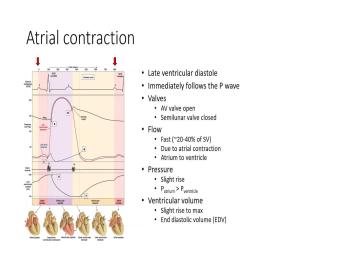
| 33:57 | now is because of the essay. , we're gonna have the S a |
|
| 34:01 | fire, and that's going to create contraction of the atria. Alright, |
|
| 34:07 | this is late ventricular diastolic, and leading into atrial sisterly. Alright, |
|
| 34:14 | here again is where we are. can see there is the P wave |
|
| 34:18 | that deep polarization. When that what happens to the pressure when I |
|
| 34:23 | on the atrial? What happens to pressure inside? It increases. So |
|
| 34:27 | a slight rise in the pressure and pressure inside the atrium goes up. |
|
| 34:31 | it greater than the pressure inside the chart? says yes. And it |
|
| 34:35 | because the ventricle is still in So what we do is we see |
|
| 34:40 | blip, and you can see right . Look at how it rises |
|
| 34:44 | Right? And because I'm squeezing whatever happens to be inside the atria, |
|
| 34:49 | now squeezing it out, as opposed allowing it to trickle through. I |
|
| 34:53 | this slight bump of volume inside the that also is represented in an increase |
|
| 35:01 | pressure inside the ventricles. Well, right. And you can see that |
|
| 35:07 | right there. Now the A V is still open, all right, |
|
| 35:13 | the pressure is greater. Yes, semi lunar valve still close because the |
|
| 35:19 | inside the aorta is significantly greater than pressure is down there inside the |
|
| 35:24 | the ventricle. All right. the flow of blood is very, |
|
| 35:29 | quick at this point. All Think about you. Have a |
|
| 35:33 | You know, you dunk in the and you pull out, pull it |
|
| 35:36 | . Water drips out of the right? What happens when you squeeze |
|
| 35:40 | ? Water come out faster? it's the same principle. Okay, |
|
| 35:44 | what you're doing is you're squeeze getting the fluid forward. That's why it's |
|
| 35:49 | now the volume of blood. At point, I'm gonna race income. |
|
| 35:52 | slide right here reaches the maximum that's enter into the ventricle. We have |
|
| 35:58 | name for it. Alright. It's the in diastolic volume E T. |
|
| 36:03 | . So it's at the end of because the diocese referring to here is |
|
| 36:07 | diastolic, so e TVs in diastolic , It is the maximum volume that |
|
| 36:12 | gonna be found in the ventricle. we've had the atria contract. That |
|
| 36:19 | moves from the s. A note the A V node Thievy note now |
|
| 36:23 | its signal down the bundle of hiss the per Kinji fibers. Right? |
|
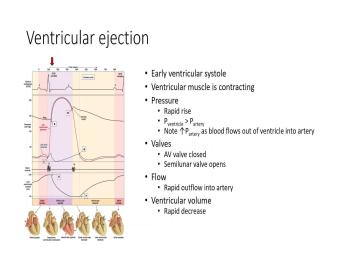
| 36:27 | so we're now entering into ventricular This is that Q r s |
|
| 36:33 | The signal goes down and then back and around so down the bundle of |
|
| 36:37 | around the back injury fibers. So why we get this really cool wave |
|
| 36:41 | it goes down, up, like that, Right? And so |
|
| 36:46 | you've got the muscle contracting. All , But when the muscle contracts, |
|
| 36:51 | gonna reach resistance. You're gonna or resistance, right? because there's fluid |
|
| 36:55 | that chamber. The chamber doesn't want collapse like a balloon. It wants |
|
| 36:59 | resist because there's a volume of fluid it, All right. And so |
|
| 37:04 | happens is the muscle begins contracting and starts building up tension. All |
|
| 37:10 | Just like when you are squeezing on bottle. When you squeezed on your |
|
| 37:14 | , you built up tension. You keep building up more and more and |
|
| 37:16 | attention. And that's what's happening is . Now see that tension increasing. |
|
| 37:23 | that red line now? Obviously the the ventricle overcomes the pressure, the |
|
| 37:30 | and the ventral overcomes the pressure in atria. So what happens is is |
|
| 37:35 | A V valve slam shut blood? don't want blood to go back to |
|
| 37:39 | Atria. You wanna keep it in ventricle, right? Because you want |
|
| 37:42 | project it out of the ventricle into arteries, right to systemic circulation. |
|
| 37:46 | the A V valve slams shut as result. Now you're gonna have massive |
|
| 37:53 | buildup. So you're going to squeeze squeeze and squeeze and squeeze and |
|
| 37:58 | You're gonna keep squeezing upward. But the semi lunar valve has it. |
|
| 38:03 | haven't overcome the pressure of the The semi lunar valve never opens or |
|
| 38:09 | open. At this point, I say never shouldn't say never. |
|
| 38:13 | the volume doesn't change. So this why it's an ISO volumetric contraction and |
|
| 38:18 | the pressure is building up once the reaches its apex. In other |
|
| 38:25 | the pressure in the ventricle overcomes the in the aorta. That's gonna be |
|
| 38:32 | that semi lunar valve opens right When pressure is greater inside the ventricle than |
|
| 38:37 | is in the aorta, blood is wanna move out, and so it |
|
| 38:40 | move very, very quickly out. so that's what you're seeing is that |
|
| 38:44 | as it drops out? Alright, valve still closed because you want to |
|
| 38:50 | the fluid in a specific direction and what happens once that valve opens, |
|
| 38:57 | ? You have the valve opening It's actually that sound is a result |
|
| 39:01 | this valve slamming shut the bump. the A V valve slamming shut |
|
| 39:06 | And then over here this will be semi lunar valve slamming shut in the |
|
| 39:11 | . Those air the sounds all but in essence, what you have |
|
| 39:14 | is Look, the valve opens the pressure still rises inside the |
|
| 39:19 | Why I've overcome my resistance now can squeezing to the point where the muscle |
|
| 39:24 | to its full contracted state. I'm all those blood out into the aorta |
|
| 39:29 | , if I'm on the right side the heart into the pulmonary artery. |
|
| 39:32 | now that artery, which is expands outward and fills up like a |
|
| 39:37 | . And so what's happening is you're more and more volume that can't leave |
|
| 39:41 | it's like a balloon. You're increasing pressure inside the aorta as well. |
|
| 39:45 | notice if you look very closely that black man sits underneath the little red |
|
| 39:50 | , doesn't it? So the pressure the ventricle is slightly above the pressure |
|
| 39:55 | the order. That's why blood continues flow out, and that is ventricular |
|
| 40:01 | . And it continues on right until muscle decides to relax, because then |
|
| 40:08 | you're in ventricular diastolic. So in ventricular sisterly, you still see a |
|
| 40:14 | contracting. The pressures are starting to a little bit because fluid is leaving |
|
| 40:19 | , but you're reaching the point where squeezed everything I can out of the |
|
| 40:25 | . So there is. Whatever is over is what is called the in |
|
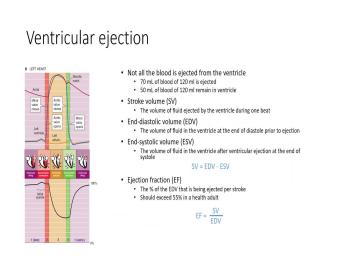
| 40:30 | volume. Now we're going to see the slide a little bit later that |
|
| 40:34 | maximum volume you can have inside the about 120 mils. Alright, You |
|
| 40:40 | about 70 mils of that blood. mil stays inside the heart. |
|
| 40:47 | So for each cycle, you're not all the blood out. It's not |
|
| 40:51 | completely. So the in systolic volume tells you the amount of blood that's |
|
| 40:57 | over after a contraction. All And so what you're seeing here, |
|
| 41:02 | drop in pressure is a function of leaving out of the aorta. So |
|
| 41:07 | pressure is dropping and you don't and the muscle begins to start relaxing |
|
| 41:11 | ventricles as well. All right, here again, we are in ventricular |
|
| 41:16 | . A V valve is closed. valve is open. Blood is moving |
|
| 41:21 | until it reaches that low point of S V. All right and again |
|
| 41:29 | and it slows down. You could rapid and slows down there as |
|
| 41:36 | So let's kind of look, that's next slide. There it is. |
|
| 41:38 | , there's those numbers I just talked . Okay, so we start off |
|
| 41:44 | blood into the ventricle. That's the diastolic volume. That's the maximum volume |
|
| 41:48 | ventricle is gonna hold. We contract push the blood out. What's ever |
|
| 41:53 | behind is called the in systolic If you take the in diastolic volume |
|
| 41:58 | subtract from it the in systolic volume tells you how much blood you ejected |
|
| 42:03 | the heart and the word we use that is called the stroke volume. |
|
| 42:07 | ? So stroke volume equals E T minus E s v. And |
|
| 42:12 | where do we see the SV Remember, we had cardiac output equals |
|
| 42:16 | heart rate, times the stroke All right. Now, the ejection |
|
| 42:26 | should be about, um um a bit over 55%. It shows you |
|
| 42:31 | a healthy individual. You can calculate out. You basically take the stroke |
|
| 42:34 | divided by the total volume. The . T. V. And that |
|
| 42:38 | tell you your ejection fraction. So healthy person is ejected at least 55% |
|
| 42:44 | the blood out of their heart with stroke. Yeah, so far you |
|
| 42:49 | with me First stage was late. asleep. Dia Stasis was what we |
|
| 42:55 | to it. Then we had the , a volumetric contraction. Then we |
|
| 42:58 | a ventricular sisterly. We had a stages in there that just to distinguish |
|
| 43:03 | it's not always just one big And then lastly, we come back |
|
| 43:07 | to the isil volumetric relaxation phase. what we have going on here? |
|
| 43:11 | where that ventricular muscle is relaxing as relaxes the pressure inside that chamber |
|
| 43:18 | which is what we're seeing right Right As it comes down, it's |
|
| 43:22 | . The pressure inside the area is coming down. Why? Because we |
|
| 43:26 | the blood is leaving through the other , right? But at a certain |
|
| 43:31 | during that period of relaxation, the inside the aorta doesn't drop us fast |
|
| 43:37 | . The pressure inside the ventricle of ventricular pressure is dropping the fastest. |
|
| 43:42 | so eventually what will happen is the . The semi lunar valve will slam |
|
| 43:47 | because the blood in the order Oh, look, there's a path |
|
| 43:50 | least resistance backwards, and it tries go back, and that's going to |
|
| 43:53 | the semi lunar valve to close. right, So when the arterial pressure |
|
| 43:59 | greater than the ventricular pressure, that's the simulator valve closes, and then |
|
| 44:05 | muscle continues to relax, Right? there's your pressure dropping, and then |
|
| 44:13 | , in the next phase, it's drop to the point where the pressure |
|
| 44:16 | lower. Now, I just ejected out of the heart. That blood |
|
| 44:21 | on the blood in front of which pushes on the blood in front |
|
| 44:23 | it all the way back around to heart. So what's gonna happen to |
|
| 44:26 | blood on the atrial side? It's to move into the atrium, |
|
| 44:30 | Yeah. And then what's gonna happen the pressure As that blood flows into |
|
| 44:34 | atrium, it goes up right. you're starting to build up pressure inside |
|
| 44:39 | H here and you can see right . That's what's going on. That |
|
| 44:43 | is rising, so the pressure in atrium is beginning to climb. The |
|
| 44:49 | in the ventricle is beginning to At some point, they're gonna have |
|
| 44:52 | cross, all right. And when cross, that's when you're gonna open |
|
| 44:55 | that valve again. So we had question online. What was that? |
|
| 45:01 | exercise? Do you? No, gonna change. And we're gonna talk |
|
| 45:10 | that a little bit later. So question was, does the does the |
|
| 45:14 | volume stay the same? Is that essence, what you're asking? You |
|
| 45:17 | , the stroke volume stay the same I'm exercising or if I'm resting or |
|
| 45:21 | , that stuff is going to be . But because the heart is trying |
|
| 45:26 | maintain or the body's trying to maintain constant cardiac output, modifications and stroke |
|
| 45:31 | are also going to result in modifications heart rate. Alright. And what |
|
| 45:35 | gonna see the very last slide in lecture deals with different ways that the |
|
| 45:40 | manages stroke volume, um, in to different activities. So it's a |
|
| 45:47 | question to ask, right? you know, I mean, you |
|
| 45:50 | know this, right? I you go and exercise, your heart |
|
| 45:53 | goes up right, because you increase need. But what is your What |
|
| 45:56 | your heart feel like when you just sprinted really hard? It's like pounding |
|
| 46:02 | of your chest, right? So it's doing is it's actually increasing stroke |
|
| 46:07 | to get Mawr fluid out per even though, in order to meet |
|
| 46:12 | needs of the body also has to the heart rate as well. So |
|
| 46:16 | two factors air increasing. And so allows for even greater cardiac output than |
|
| 46:21 | would normally think. If I'm only one or the other or both of |
|
| 46:25 | are being adjusted. Have I answered question? Okay. All right. |
|
| 46:31 | the last phase is we're kind of back to where we started. This |
|
| 46:35 | where we're gonna start refilling the So this is a little bit before |
|
| 46:39 | DIA Stasis, right? So we the the pressure inside the atria was |
|
| 46:47 | . We said the pressure inside the was dropping and they basically cross over |
|
| 46:52 | other. When that happens, when pressure inside the atria becomes greater than |
|
| 46:56 | inside the ventricle that causes the valves open up the A V valve. |
|
| 47:02 | the AP valve open ups blood, has been building up inside the |
|
| 47:06 | You're basically opening up, you basically spill directly into the ventricle. |
|
| 47:11 | because the pressure inside the venture inside atria remains higher than the ventricle. |
|
| 47:15 | valve remains open, so we initially off with a fast flow. But |
|
| 47:21 | it kind of slows down. Kind like if you take a cup or |
|
| 47:25 | and you spill it the majority, fluid comes out at the front |
|
| 47:29 | and then the rest of it kind trickles out. That's kind of what's |
|
| 47:32 | on here is it's trickling in, so the rate of flow into the |
|
| 47:37 | slows down over time. But as as you have the ventricle in its |
|
| 47:43 | state and the atria is in, pressure inside, the tree is |
|
| 47:47 | That's gonna allow the flow. So , blood is basically going from the |
|
| 47:51 | into the atria, just kind of as it goes through and enters directly |
|
| 47:55 | the ventricles, so notice it's The flow of blood in the ventricle |
|
| 47:59 | not dependent upon the atria of It's just dependent upon the pressure, |
|
| 48:04 | the fluid from the circulation through the directly into the ventricle. Does that |
|
| 48:11 | sense a little bit now, why is a new, interesting strategy. |
|
| 48:18 | this works is because this allows us change our heart rate all right, |
|
| 48:25 | really kind of mucking up how much our heart gets. So, I |
|
| 48:29 | , we got these periods of Alright, so right now you guys |
|
| 48:33 | sitting around your slowly falling asleep to nice sound of my sweet voice. |
|
| 48:38 | should talk a little bit deeper and little bit more soothing so that you |
|
| 48:43 | feel a little bit better while we sitting here. You might want to |
|
| 48:46 | out your lights, guys at All right, So what happening is |
|
| 48:50 | heart rate slows down, right? like thumb, thumb, some thumb |
|
| 48:55 | , thump, thump, thump. . So the diastolic period is pretty |
|
| 49:02 | , but you can increase your diastolic , right? We bring shafts in |
|
| 49:07 | room and say everything has to go . You know, all of a |
|
| 49:10 | your heart rate is gonna go up quick. It's gonna thump. |
|
| 49:12 | thump, thump, thump, thump, thump, thump. |
|
| 49:14 | You just shorten your diastolic time, ? You didn't change your systolic |
|
| 49:19 | You change your diastolic time. Now is a slight change systolic, but |
|
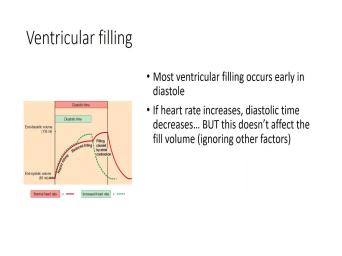
| 49:23 | not gonna worry about that right All right, but because ventricular filling |
|
| 49:29 | based on that type of physics, ? Most of my feeling of the |
|
| 49:34 | occurs on that front end, Because it's building up inside the A |
|
| 49:40 | . You open up the valve. of that blood jumps in, you |
|
| 49:42 | , just spills over into the And so the rest of that |
|
| 49:47 | right? So if you if you about it, look at this point |
|
| 49:51 | here, all right? This is line we're looking at. How much |
|
| 49:55 | in my feeling during that trickle time I just kind of outlined there Very |
|
| 50:01 | , right? I mean, if is 100% Phil, there's your |
|
| 50:06 | Going from here to here is, , what, 5%? Maybe 10% |
|
| 50:10 | the blood is kind of trickling right? And then the remaining portion |
|
| 50:17 | squeezing in when the atria contract. what that blip is, right? |
|
| 50:24 | blip right here, that's when the contract I get that blip of I'm |
|
| 50:28 | you out. So very little is during those latter stages of the passive |
|
| 50:36 | . All right, so when I my heart rate and reduce my diastolic |
|
| 50:41 | really, all I'm missing out on this little bit flowing in on its |
|
| 50:47 | passive nature? Instead of waiting for , Thio slowly trickle in. I'm |
|
| 50:54 | it in. I'm using the atrial to contract to push it in so |
|
| 50:58 | don't lose the volume. I just the time and I don't need the |
|
| 51:02 | . The time is is a just period that allows for rest occur That |
|
| 51:11 | me to make adjustments to my heart . Okay, So fill volume is |
|
| 51:19 | affected because of the natural physics that of blood. Kind of accumulating in |
|
| 51:24 | atria during that systolic period, the systolic period. And then when you |
|
| 51:30 | into ventricular, die asleep, you the most of the fluid in, |
|
| 51:34 | the rest kind of just trickles in the last little bit of a squeeze |
|
| 51:38 | . Okay. So far, how doing? Are you okay? That |
|
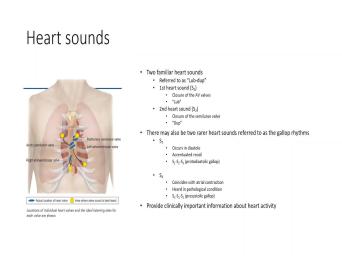
| 51:47 | people too sweet. Sleep. All . Heart sounds, heart sounds represent |
|
| 52:02 | sounds of the valves. Clothing. right. The way I like to |
|
| 52:07 | this to people just so you can it, uh, your your heart |
|
| 52:10 | a room, you know, write rooms and your blood is an angry |
|
| 52:19 | , right? Do you remember being angry teachers you can't tell me or |
|
| 52:23 | teenage? You can't tell me what do. Slam. That's what's |
|
| 52:28 | Slam slam. It's just those doors . All right, So the first |
|
| 52:36 | y'all, if you've all heard the , right, if you haven't go |
|
| 52:39 | somebody on the street randomly say, still and then just put your head |
|
| 52:43 | their heart, they won't mind. won't think you're crazy, right? |
|
| 52:49 | you're here. It's loved up. up, loved up. Looked up |
|
| 52:53 | sound. That bump bump is slam . All right, slamming the A |
|
| 52:58 | valve closed ventricular contraction, right. the blood out blood wants to come |
|
| 53:05 | in slam again, assuming lunar valve or aortic valve. If you're looking |
|
| 53:10 | the left side of the heart, all this. Now some of you |
|
| 53:14 | lucky and have extra hearts or not hearts. That would be really |
|
| 53:19 | You know, you have extra heart and they're galloping rhythms. Um, |
|
| 53:24 | worry about them so much. I asked questions about thes. It's these |
|
| 53:27 | . If I'm gonna ask you gonna be What are those two? |
|
| 53:29 | are those two sounds? Mhm. we listen to the heart sounds. |
|
| 53:37 | you went to the doctor at the of the year before you started school |
|
| 53:40 | everyone is supposed to. All Get yourself checked out. Make sure |
|
| 53:44 | don't carry any sort of strange viruses anything on a campus. I don't |
|
| 53:52 | . What do you do? Do listen to your heart? What do |
|
| 53:57 | say? Breathe. Breathe. Hold your breath. Right. What |
|
| 54:00 | you doing there? Just listen to your heart's doing right, And they |
|
| 54:03 | that primarily. Just kind of determine or not your hearts in good |
|
| 54:08 | All right. Now, obviously, my heart pushes all that blood |
|
| 54:15 | it creates a pressure wave in the . And because of the way the |
|
| 54:19 | work directly outside the heart, their . We're gonna learn more about this |
|
| 54:22 | a coming lecture. When we talk the vein, what happens? Our |
|
| 54:26 | and the veins. What's gonna happen that the aorta expands. And so |
|
| 54:30 | creates this pressure, Bullis. And uses that pressure boats to drive |
|
| 54:34 | And so you actually can look at pressure inside the aorta, and it |
|
| 54:38 | like it has a systolic and diastolic , Right? It's not as large |
|
| 54:44 | the, uh, the, uh . Remember, we saw that on |
|
| 54:49 | previous lecture where literally was like, . Zero. Here's 1 20. |
|
| 54:53 | was going up and down like so that would be the ventricle. |
|
| 54:57 | ? But in the aorta, it's going between those two points at |
|
| 55:00 | 20 and 80 right? Because there's blood inside the aorta, right? |
|
| 55:06 | then that pressure is really pulse a for a long period of time, |
|
| 55:11 | . So have you ever tried to your heart rate by putting your fingers |
|
| 55:16 | your wrist or on your neck? maybe over here? Have you felt |
|
| 55:21 | who have tried that? Alright, you have it, well, you |
|
| 55:25 | go home and do it now. do you do it now? I |
|
| 55:27 | care. Yeah? Can I have find it right? You know, |
|
| 55:32 | is the hard one, right? you can feel it, you |
|
| 55:34 | Yeah, I can feel the thump , thump thump. Right. That's |
|
| 55:39 | the pressure that Z being pushed through arteries by that Boulis of blood through |
|
| 55:47 | body. But as you move further further away from the heart and you |
|
| 55:51 | encountering the smaller and smaller arteries, not quite as elastic they have. |
|
| 55:58 | basically produced resistance, and it removes pulse little wave. So what you |
|
| 56:03 | up with is mawr smooth flow instead , ah, flow that's going up |
|
| 56:07 | down a pulse. It'll flow And so that's kind of what this |
|
| 56:11 | of this thing is showing you. can see here is the pulse. |
|
| 56:14 | is all the way, and then you get down here and it's like |
|
| 56:17 | no pulse. It basically it becomes smooth slope. That's just the representation |
|
| 56:24 | there's higher pressure here. Lower pressure , And it's there is that resistance |
|
| 56:28 | not allowing you to have that pulse it doesn't expand and contract, all |
|
| 56:33 | , it lacks the complicity or the , I guess is the correct |
|
| 56:38 | all right. And as you move and further away right, you get |
|
| 56:42 | , smaller structures which have greater which produces less flow. In other |
|
| 56:48 | , the pressure great. It drops more rapidly and the flow becomes more |
|
| 56:54 | . But again, if you look this chart, you know, here |
|
| 56:57 | am over in the aorta, there's mean arterial pressure. Here I am |
|
| 57:03 | in the Vienna Cavell. That's low . And even though that goes all |
|
| 57:07 | way around my body, is there pressure? Grady Int If this is |
|
| 57:13 | pressure over here in the order, this is my pressure down there and |
|
| 57:16 | Kiva is there pressure? Radiant? , that's where the blood want to |
|
| 57:21 | to the vena cava. That's because it's naturally flowing down its pressure |
|
| 57:27 | . Alright, so there is a wave that is occurring in the |
|
| 57:32 | It's easy to see, but it over the Kapler's in the veins. |
|
| 57:36 | , typically, what we say, is no pressure wave in the |
|
| 57:39 | But the truth is, is, you move into the more advanced |
|
| 57:44 | you'll see that there is not a wave of a pressure wave in the |
|
| 57:50 | . But we create these unique pressure on the Venus side of the |
|
| 57:57 | All right, so they lack a pulse. But we have factories that |
|
| 58:03 | them and what we have is we these air kind of cool. There's |
|
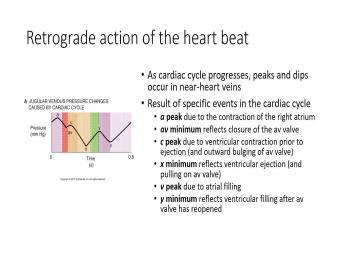
| 58:05 | retrograde activity of the heart, the pump and the skeletal pump. All |
|
| 58:13 | , so this one is the least . Do not memorize any of these |
|
| 58:16 | things. I'm not asking you to the primarily because look at the time |
|
| 58:20 | on this less than a second, . And this is basically looking specifically |
|
| 58:25 | the jugular vein, right? So gonna be different in different areas. |
|
| 58:29 | what we have here basically says, , when the heart contracts, what |
|
| 58:34 | gonna do, So we're meant when ventricle contracts, you have the aorta |
|
| 58:37 | top. When it contracts, it's pressure, which is going to cause |
|
| 58:41 | aorta or not the sort of the to kind of expand and contract with |
|
| 58:49 | . Well, that's gonna be effect the vein that's attached to it, |
|
| 58:52 | ? The vena cava. So if caused the order to expand outward, |
|
| 58:56 | creates a drop in pressure inside the , right? Which is gonna drive |
|
| 59:01 | fluid from the veins. Right. if I contract the atrium right, |
|
| 59:06 | I'm gonna do is I'm squeezing and I'm creating back pressure, and |
|
| 59:10 | builds up pressure inside the vein. so what I'm doing is I'm basically |
|
| 59:14 | and relaxing in a micro scale, basically creates these small pressure gradients that |
|
| 59:20 | fluid forward or allow pressure to build so fluid can drive forward once relaxation |
|
| 59:26 | . So when the heart contracts, not just pushing blood, it's pulling |
|
| 59:33 | . That's what I want you to about it. All right? That's |
|
| 59:36 | the retrograde action of the heart So we don't have a push pump |
|
| 59:42 | . We also have a pool pump for the cool one. I think |
|
| 59:46 | is the coolest one respiratory pump. right, now we're gonna talk about |
|
| 59:53 | again. So people at home, can do this without fear of looking |
|
| 59:57 | an idiot. People in the I want you to look like an |
|
| 60:00 | with me. Put your hands on on your chest. I'm not saying |
|
| 60:04 | your chest. I'm saying on your right where your ribs are. All |
|
| 60:09 | ? I want you to feel when breathe in breathe, do a deep |
|
| 60:13 | and then breathe out. Do you the rise and fall of your rib |
|
| 60:20 | . All right, you're bellows, ? And that's what we talk about |
|
| 60:23 | we talk about breathing, right, gonna use that example over and |
|
| 60:26 | When we talk about respiration, you're a bellows. Alright, So what's |
|
| 60:29 | is is I'm expanding the thoracic all right? And then I'm compressing |
|
| 60:34 | thoracic cage when I breathe in Breathe out. Compression. Alright. |
|
| 60:40 | if I'm expanding the thoracic cage, increasing the volume inside the thoracic |
|
| 60:45 | which also results in a drop in . Right? That drop in pressure |
|
| 60:52 | relative to the abdominal cavity. Because I breathe in and we're sorry when |
|
| 60:57 | breathe in, right, I'm pushing my diaphragm, which pushes down on |
|
| 61:02 | abdomen. Right. So I'm reducing volume in my abdominal space. And |
|
| 61:07 | I'm reducing the volume of my abdominal , what am I doing with the |
|
| 61:10 | in the increasing it? So when breathe in dropping pressure in my |
|
| 61:16 | increasing pressure in my stomach, what's do it's going to push blood from |
|
| 61:21 | belly, right? That's moving towards heart towards the heart faster, |
|
| 61:27 | You see that? Expanding this pressure down, pushing on this pressure goes |
|
| 61:34 | and so drives it that way. right, then, when I breathe |
|
| 61:37 | , what do I do? I greater pressure here, which is basically |
|
| 61:43 | upward here, which creates a volume in the abdomen, which pulls |
|
| 61:48 | Blood up towards the abdomen allows pressure build up as blood accumulates in the |
|
| 61:55 | veins. Right. But at the time, I'm pressing on my chest |
|
| 62:00 | I press on my chest that propels blood towards the atrium, so just |
|
| 62:06 | is a secondary pump. It's not strong pump, but it's a pump |
|
| 62:12 | . And so what you're doing is sucking to the stomach, pushing to |
|
| 62:15 | chest, sucking to the stomach, to the chest over and over and |
|
| 62:19 | again. Just a function of Trying to call. I think it's |
|
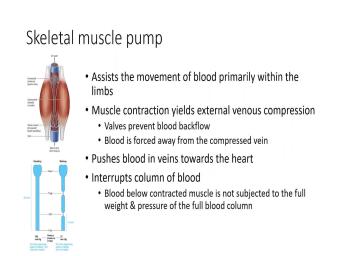
| 62:24 | . All right. Third, pump skeletal muscle pump. All right, |
|
| 62:31 | all sitting down. E want you to contract your quads and your, |
|
| 62:36 | , calves. All right. You propelled blood to your heart. Moving |
|
| 62:44 | blood to move to your heart. , Most your veins or deep |
|
| 62:48 | They're not superficial, superficial veins or ones on the surface. Deep veins |
|
| 62:53 | usually found inside, not inside the but surrounded by muscles. The word |
|
| 62:58 | want to kind of use here. right. Now, if you think |
|
| 63:02 | the way your body is alright, basically one big giant structure has the |
|
| 63:08 | at the top and you have a that goes right to it, |
|
| 63:10 | So it's basically a column of All right. Now you can imagine |
|
| 63:15 | the bottom of that column that blood down there. That small unit of |
|
| 63:19 | is holding the unit above above which is holding the unit above, |
|
| 63:23 | above it yada, yada, yada, yada. So, down |
|
| 63:26 | at the bottom, what's the pressure that high or low? It's |
|
| 63:32 | right? If you've ever gone scuba , right, you can You can |
|
| 63:35 | . And then the deeper and deeper go, the greater the pressure |
|
| 63:38 | Basically, you have all that water down on top of you, all |
|
| 63:43 | . It's buoyant, but it's still , and so you can imagine the |
|
| 63:48 | it takes to get your blood from little toe up to your up to |
|
| 63:52 | heart is gonna be a lot of . So one of the ways that |
|
| 63:56 | body accomplishes this is it's gonna break that column. Now, we're gonna |
|
| 64:00 | here in a moment that they are not in the moment. But in |
|
| 64:03 | lecture is that veins have valves in . That's that's one way that it |
|
| 64:07 | up the columns. So you have a valve every couple of centimeters. |
|
| 64:11 | you're really not carrying the full weight blood on that column? It's basically |
|
| 64:16 | that small little immune it whatever from to valve. But how do you |
|
| 64:21 | blood to move forward if you don't a lot of pressure? So I'm |
|
| 64:24 | gonna make up numbers. Is it if I make up numbers? All |
|
| 64:27 | . So imagine the blood pressure in in the in the the capital, |
|
| 64:32 | side of the or the Venus side a cap players around 10 millimeters of |
|
| 64:37 | . The blood pressure inside your atria about zero millimeters of mercury. So |
|
| 64:42 | slope to go from your little toe your heart is like nothing, |
|
| 64:49 | I mean, that's a 10 millimeter difference, considering that the pressure difference |
|
| 64:55 | the systolic and diastolic is 40 millimeters mean, you're looking at a |
|
| 64:58 | That's, you know, like, steep. You guys can't see |
|
| 65:01 | I'm making a steep slope with my and a very shallow slope. So |
|
| 65:07 | have to that has to overcome which by itself, is gonna be |
|
| 65:10 | difficult. So the way that your does that is just squeeze the |
|
| 65:14 | right. If I squeeze the fluid has no choice but to go |
|
| 65:19 | with one way valves, right? so when you sit down when you |
|
| 65:23 | , when you walk, when you when you gesture, everything you're doing |
|
| 65:26 | muscle squeezing on these veins, which propel the blood back towards the |
|
| 65:31 | It's really obvious in the legs, when you squeeze, you can move |
|
| 65:36 | you know, you're you're really feeling against gravity. Not so much in |
|
| 65:39 | arms, but it's still doing it as well. All right, all |
|
| 65:50 | . So cardiac muscle. We've talked it in terms of structure, so |
|
| 65:55 | nothing really new there. I do to point out the heart in terms |
|
| 65:58 | its structure, is actually kind of . We've got two little things |
|
| 66:01 | First off the left ventricle, Left is on this side. The |
|
| 66:05 | very, very thick versus the right , which is very, very |
|
| 66:08 | The reason being is just by virtue how much blood I have to |
|
| 66:12 | Right. Pulmonary circulation is basically about of my body. Systemic circulation is |
|
| 66:18 | 80% of my body, right? the amount of blood that needs to |
|
| 66:21 | moving right. So remember, my is pumping blood. It still has |
|
| 66:25 | move all the blood back around to heart. So it's gonna be doing |
|
| 66:28 | lot more work. That's why the ventricle is thicker. Alright. |
|
| 66:32 | so what we say is right low resistance, low pressure to overcome |
|
| 66:37 | ventricle, high pressure, high resistance overcome. All right. The other |
|
| 66:42 | that's kind of cool is how your develops its develops as a spiral |
|
| 66:46 | So when your heart contracts, even you have a tree in the |
|
| 66:49 | what is doing is it's ringing in heart. All right, so if |
|
| 66:54 | ever milt in animal like a cow goat, a sheep no small |
|
| 67:04 | It's funny, right? Sorry. was a fan of The Simpsons and |
|
| 67:10 | time ago, uh, they discovered at The Simpsons at the school that |
|
| 67:15 | weren't drinking milk. They were drinking . And what Mulk was was rat |
|
| 67:21 | , and they went down. And was the mob that was selling it |
|
| 67:25 | him. And they had, a like, just cages of rats |
|
| 67:30 | up the little time milking. that was funny. I'm sorry. |
|
| 67:36 | right. So when you think about a towel all right, when you |
|
| 67:40 | a towel, what do you do that? That's what the heart's |
|
| 67:43 | And it's and what that does. allows for the muscles to to squeeze |
|
| 67:46 | such a way to propel the blood and out through the simulator valves. |
|
| 67:52 | right, And this is just kind showing you that arrangement. How How |
|
| 67:55 | looks like, um, there's a of information on these two slides here |
|
| 68:01 | you don't need to know. I to try to teach it and realize |
|
| 68:04 | always run out of time, but like to think of that. |
|
| 68:06 | What basically says is that a tree the ventricles. Work together is like |
|
| 68:10 | Atria contract. Together, the ventricles together. While that's true, it's |
|
| 68:14 | 100% true that there are off sync just a little bit. And that's |
|
| 68:18 | that those grass are really trying to you. That's not so important to |
|
| 68:22 | . I just mentioned it. I'm gonna ask you on the test. |
|
| 68:26 | , what you should be aware of what does cause each of the individual |
|
| 68:32 | . So there's some detail in there that becomes important. Um, this |
|
| 68:37 | is exact. Same thing on git you how the heart actually does |
|
| 68:42 | So when the ventricle contracts, it's of like squeezing toothpaste. You |
|
| 68:46 | where your propelling it up? Because whole round structure contracts, whereas on |
|
| 68:51 | right side of the heart, it's like a bellows where it's squeezing in |
|
| 68:55 | this direction towards. So it's just little bit slightly different in terms of |
|
| 69:00 | two types of contractions, not particularly , the cardiac muscle contraction we said |
|
| 69:10 | is dependent upon calcium. We've learned what I wanna talk to you about |
|
| 69:14 | quickly here is how do we regulate . So we're gonna regulate at the |
|
| 69:18 | of troponin and we're gonna be regulating at the level of circa. |
|
| 69:24 | That little molecule I just circled right is called fossil Lam Binh. |
|
| 69:29 | see? It's gonna be on the slide, so I'm just trying to |
|
| 69:32 | you where it's at. Fossil right? What fossil ramen is is |
|
| 69:39 | in Hibbert inhibitor of circa? It's brake pedal on circuit slows thetacticsroom circuit |
|
| 69:44 | . Remember what circuit did circus the in a platinum particular calcium pump So |
|
| 69:50 | pumps. It allows for calcium be out of the of the cytoplasm. |
|
| 69:58 | . And what fossil Lam Binh does because it's an inhibitor. If you |
|
| 70:02 | for related, What happens is you the inhibitor. So as you fost |
|
| 70:07 | late, it's going to increase the of relaxation all right. And the |
|
| 70:13 | thing is going to be true Um, if I fast for |
|
| 70:17 | um troponin tie, it allows it causes tnc which binds up calcium |
|
| 70:24 | release um um to release calcium, means you're able to go through a |
|
| 70:30 | faster, allows relaxation to occur so there's I'm just trying to show |
|
| 70:38 | There's some ways that we regulate I think that's what this does. |
|
| 70:42 | brings us down to our last three . All right, so much of |
|
| 70:49 | we're talking about today is just the cardiac cycle. And ultimately, with |
|
| 70:53 | cycle, you're creating a volume of that's being ejected. That's your stroke |
|
| 70:58 | , Alright? And so how do affect stroke volume? One of the |
|
| 71:01 | that we could do to make stroke change. All right, There's three |
|
| 71:06 | . We could do it on the end. We could do it on |
|
| 71:07 | back end. Or what we can is we can alter the degree of |
|
| 71:11 | Il ity of the heart. So front and back end and how |
|
| 71:16 | the heart contracts. So what do mean by front line that this is |
|
| 71:19 | pre load how much blood we returned to the heart. And if you |
|
| 71:23 | your text book, you read all Frank Sterling, and you probably stared |
|
| 71:27 | that for a little while. You're , I don't know, I don't |
|
| 71:29 | . I'll learn about in class, I'm gonna basically bald too boil it |
|
| 71:33 | . There's a lot of words on slide, but this is what it |
|
| 71:35 | down to. All right, Frank . There's two scientists. They examine |
|
| 71:40 | heart, and they discovered this really fact. The heart will pump whatever |
|
| 71:45 | give it. So the more blood returns to the heart, the more |
|
| 71:50 | the heart will pump less blood. return to the heart of less |
|
| 71:53 | The pump the heart will pump. an intrinsic ability, Hart, to |
|
| 71:57 | how much blood is in there. other words, it detects that |
|
| 72:01 | And the more pressure there is, harder it's gonna pump to push out |
|
| 72:04 | greater volume. All right, so you increase the amount of blood returning |
|
| 72:11 | to the heart, that's your pre . Alright, what that's going to |
|
| 72:15 | is it's going to increase how much heart pumps out, right? That's |
|
| 72:20 | stroke volume. And it does so what you've done is you've increased the |
|
| 72:24 | diastolic volume right so much you return the heart, basically, is the |
|
| 72:29 | end. And so how much I in in diastolic volume increases, that |
|
| 72:33 | the systolic volume has to increase is , that's number one. Pre load |
|
| 72:38 | number one. So if I reduce load systolic volume or stroke volume goes |
|
| 72:46 | because in diastolic volume goes down the same thing. All right? |
|
| 72:50 | after load. This is what you're familiar with. All right. High |
|
| 72:55 | pressure. If other words. If if my blood pressure is high. |
|
| 72:58 | resistance to pushing blood into the the heart is gonna have to work |
|
| 73:02 | . Does that make sense? The crap you have in your closet, |
|
| 73:05 | harder it is to get stuff into . Same principle here. Alright. |
|
| 73:10 | as my after load increases, what gonna do is that's going to increase |
|
| 73:15 | system. The in systolic volume, basically serves as a point of |
|
| 73:20 | My heart has to work harder. what ends up happening is is my |
|
| 73:23 | volume goes down. This is why dangerous for the heart. That's one |
|
| 73:27 | why it's dangerous for the heart to high blood pressure because your heart's now |
|
| 73:32 | to get more volume out of All right, so this results in |
|
| 73:37 | increased so basically increase increases if, load increases. Basically, it reduces |
|
| 73:42 | ability of the heart to eject That's what we're trying to get |
|
| 73:46 | All right, So it's a lower volume last one, and then we |
|
| 73:51 | to go home and then we get have a long weekend. We get |
|
| 73:54 | watch football. For those who like further, you'd like to drink pumpkin |
|
| 73:58 | in 90 degree heat. You can that. It's that time of |
|
| 74:02 | right? Pumpkin lattes, pumpkin, latte, Not pumpkin Lottie's. |
|
| 74:10 | All right. I'm on a Agents on a Tropic Agents are simply |
|
| 74:16 | external factors that alter the contract Il of the heart. All right, |
|
| 74:22 | they could be both positive and So they're those factors that are not |
|
| 74:26 | of the heart, their external to heart. So they could be It |
|
| 74:29 | be on autonomic innovation so sympathetic versus . It could be hormones that can |
|
| 74:35 | effect. It could be drugs that take those air all on a |
|
| 74:40 | Alright, so I know tropic not . Oh, so I know |
|
| 74:44 | So generally speaking, what you're gonna is if you are, If you |
|
| 74:49 | a nine a tropic agent. What does is it makes the availability of |
|
| 74:53 | change. When you make the availability calcium change, you're going to make |
|
| 74:59 | orm or cross bridges. So you less orm or contract tile strength. |
|
| 75:05 | right, so this is positive. calcium availability by increasing number of calcium |
|
| 75:14 | , you increase the number of cross . So that would be examples. |
|
| 75:20 | . Any drugs that make your heart harder? That would be an easy |
|
| 75:24 | to it. Negative. On the hand, decrease in calcium. Weaker |
|
| 75:32 | . Simple enough. Kind of, of. So if I I'm just |
|
| 75:42 | challenge you here, make you think a second and then we'll get out |
|
| 75:45 | here, I exercise my heart beats . What's gonna happen to my Venus |
|
| 75:51 | ? Go up, Go down. the same by exercise is gonna go |
|
| 75:58 | . So what happens to my Venus my venous return goes up? What |
|
| 76:03 | to my, um, e T ? It increases. So what's my |
|
| 76:09 | going to do? Put more blood harder. Okay. Excellent. That's |
|
| 76:18 | hard. Right? So that's that's kind of thing that you need to |
|
| 76:23 | thinking about here. What happens Right, you know. And |
|
| 76:27 | of course, to make the blood factor, right? My veins Excuse |
|
| 76:32 | . My arteries constrict so the blood flows faster through them to get to |
|
| 76:37 | tissues that they need to get So what happens to my after load |
|
| 76:41 | after let go up or go down my if I have arterial constriction after |
|
| 76:50 | goes up So what does my heart to do? Beat harder. So |
|
| 76:54 | mean when I exercise? I get blood to my heart, to my |
|
| 76:57 | harder. And it's harder to get blood where it needs to go. |
|
| 77:00 | my heart beat harder. So that's when I exercise my heart beat harder |
|
| 77:04 | , it's basically both of these things simultaneously. Plus, you can throw |
|
| 77:08 | all the sympathetic activity and all the and other things that are also supporting |
|
| 77:14 | . And I'm getting the hormones were to you would be things like |
|
| 77:18 | epinephrine, norepinephrine. Okay, so would be like the tough end of |
|
| 77:24 | trying to understand this stuff. But you see that application if you're sitting |
|
| 77:30 | on the sofa after running, You just went for your five mile |
|
| 77:34 | . Because I know you're all strong . You know, your heart's beating |
|
| 77:38 | , man, you go lie on sofa, put a cold, damp |
|
| 77:41 | on your head and drink a What's your heart rate gonna do? |
|
| 77:44 | gonna go down, right? Well, you no longer have that |
|
| 77:49 | stimulation. So no out of tropic that's going to reduce, um, |
|
| 77:54 | load. It's gonna reduce after All that stuff is going to go |
|
| 77:59 | as well. Capiche. Yeah. . I don't know any other. |
|
| 78:08 | is Hi there. There's Japanese. all good. Any questions from online |
|
| 78:25 | Yeah, eso eso. So the with arterial constriction, right? All |
|
| 78:33 | , so So it's again. It's . It's a broader process. I'm |
|
| 78:40 | to get you to think, trying get them to think about So when |
|
| 78:44 | the heart is beating harder when you're your being stimulated primarily through sympathetic |
|
| 78:49 | which is causing the heart to pump and harder and harder. But part |
|
| 78:53 | that sympathetic activity is going to cause constriction. The reason for that arterial |
|
| 79:00 | is we're trying to get blood faster the heart to the tissue where it |
|
| 79:04 | to go. It's not creating resistance the sake of slowing down them or |
|
| 79:09 | prevent blood. It's actually it's like your finger on the end of the |
|
| 79:13 | , right? You ever do that you're a kid trying to spray? |
|
| 79:15 | we put a finger on the end the hose. You're not there to |
|
| 79:17 | the water from coming out. You're to make the water come out |
|
| 79:20 | and when it comes out, faster further, you know, or further |
|
| 79:24 | . That's why you do that. it's the same sort of principle. |
|
| 79:27 | constriction of the arteries results in quicker , you know, flat faster flow |
|
| 79:34 | that artery. All right, So order to overcome that restriction that the |
|
| 79:39 | has to be harder to do that ? So it zey what I was |
|
| 79:45 | to get at here is there's there load that the heart must overcome during |
|
| 79:52 | in order to ensure that activity. because it's beating harder and more |
|
| 79:56 | you're also increasing pre load because you're so much more blood out they'll put |
|
| 80:03 | way. Um, your heart rate you're sitting right now is about 60 |
|
| 80:06 | per minute. Right? When you're , your heart rate could be around |
|
| 80:09 | 60 beats per minute, and you're beating harder. In other words, |
|
| 80:13 | stroke volume goes up. So you're instead of moving. Um, |
|
| 80:19 | We could do the math, but 120 million to say it's 70 |
|
| 80:23 | times 60. So what is 420. 4200 mils. We're looking |
|
| 80:30 | 4.2 mills in a minute. By my math, right are 4.2 |
|
| 80:39 | Thank you for pulling out the calculator you just checking your email 70 |
|
| 80:43 | 70 times. Um, 60 4.2 . Right. Okay, so |
|
| 80:51 | in 11 minute, your heart is . Ladies, you're almost your entire |
|
| 80:57 | of blood, right? But think when you're exercising, Alright. You |
|
| 81:03 | your heart rate to want to 160. Yes, all right. |
|
| 81:08 | let's say we increase our stroke So you're now moving, um, |
|
| 81:12 | of 70 mills, let's say 100 . I'm just making up a |
|
| 81:17 | so 16 liters of blood, So you're part is receiving mawr |
|
| 81:24 | and it's also having overcome resistance, it's working harder to do all |
|
| 81:29 | Perfect. So that's what I was to get out. That's what the |
|
| 81:35 | I'm saying is the heart is working to overcome the after load. I |
|
| 81:40 | I answered the question may have gone a rabbit trail. All right, |
|
| 81:45 | done for the day. You don't to hang out here unless you want |
|
| 81:49 | actually have a meeting with student. other than that, uh huh. |
|
| 81:54 | questions from yes, all made Just nod your head and say, |
|
| 81:59 | course, Dr Wayne is perfect All hundreds. If you have |
|
| 82:05 | don't be afraid to ask. Have great |
|